

Correlation between Systemic Lupus Erythematosus Disease Activity Index, C3, C4 and Anti-dsDNA Antibodies
- PMID: 27365721
- PMCID: PMC4920905
- DOI: 10.1016/S0377-1237(10)80118-2
Correlation between Systemic Lupus Erythematosus Disease Activity Index, C3, C4 and Anti-dsDNA Antibodies
Abstract
Background: Therapeutic decisions in systemic lupus erythematosus (SLE) are based on the disease activity and nature of organ involvement. There are various clinical and laboratory methods to assess the lupus flares.
Methods: Fifty one SLE patients with active disease (lupus flare) were studied. Systemic lupus erythematosus disease activity index (SLEDAI), C3, C4 and anti-double stranded DNA levels were estimated and repeated monthly till remission. After remission these tests were done three monthly. Values of serological parameters were then correlated with SLEDAI score.
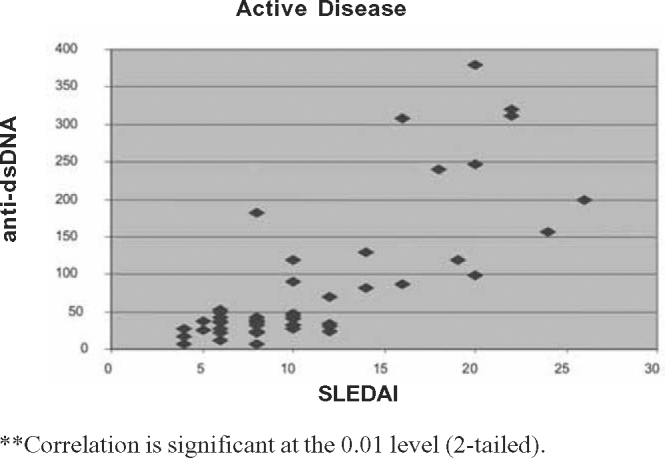
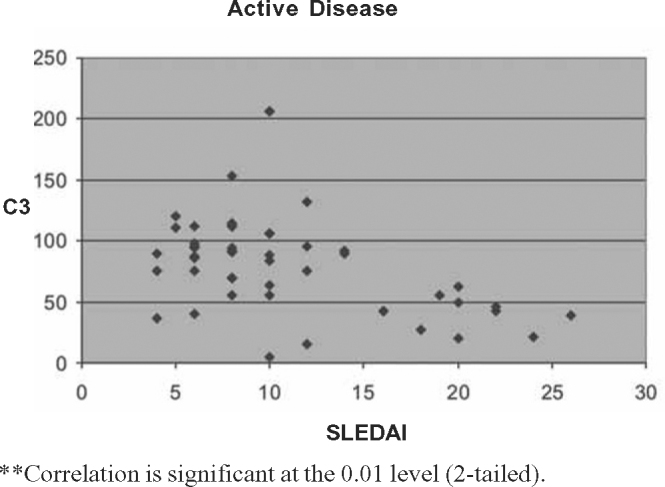
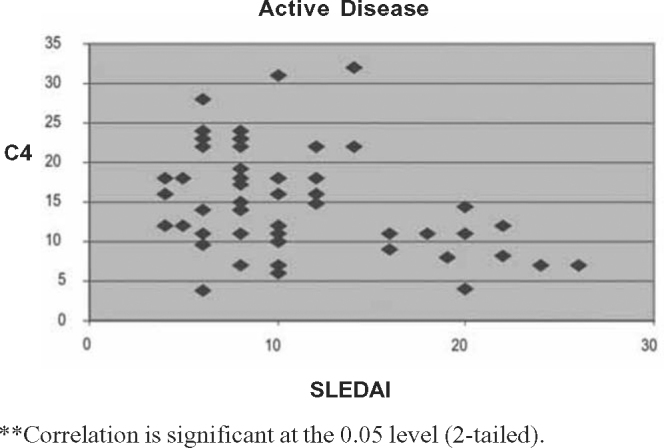
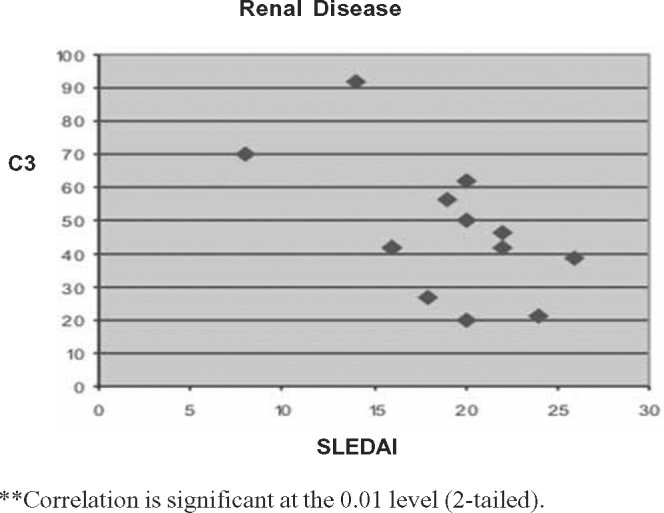
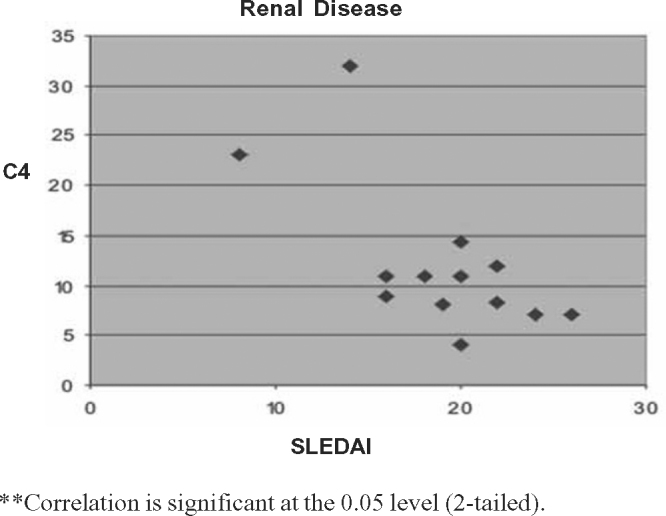
Result: Thirteen (25.4%) patients had predominantly renal involvement while 38 (74.6%) patients had non-renal affliction. Musculoskeletal and mucocutaneous symptoms were the commonest features of lupus flare (90%). It was observed that 12 out of 13 (92.3%) patients with active renal involvement had low C3 levels and 11 (84.6%) had low C4 levels. The anti-dsDNA levels were elevated in all patients with predominant renal flare. In non-renal flare anti-dsDNA titre was raised only in 35% cases. Low C3 and C4 levels were noticed in 43% and 53% of non-renal flares respectively. Significant positive correlation was noticed between SLEDAI score and anti-dsDNA levels (0.01 level two-tailed prediction) and a significant negative correlation was observed with SLEDAI and C3, C4 levels (0.01 and 0.05 levels, two-tailed prediction) in our patients. On subgroup analysis it was noticed that this correlation is stronger for renal lupus. Negative correlation of SLEDAI and complement levels was not observed in non-renal flares.
Conclusion: Calculation of SLEDAI is a vital clinical tool for assessment of SLE patients. Serial estimation of anti-dsDNA titre, C3 and C4 levels help us diagnose lupus flare and make appropriate therapeutic decisions in patients with high SLEDAI score.
Keywords: Anti-dsDNA; Complement; Lupus flare; Systemic lupus erythematosus.
Figures
References
-
- Bombardier C, Gladman DD, Hurwitz MB, Caron D, Chang CH. The committee on prognosis studies in SLE. Arthritis Rheum. 1992;35:630–640. - PubMed
-
- Gladman DD, Goldsmith CH, Urowitz MB. Sensitivity to change of 3 systemic lupus erythematosus disease activity Indices: Internal validation. J Rheumatol. 1994;21:1468–1471. - PubMed
-
- Petri M, Buyon J, Skovron ML. Reliability of SELENA SLEDAI and flares as a clinical trial outcome measure. Arthritis Rheum. 1998;41:S218.
-
- The American College of Rheumatology response criteria for SLE clinical trials: measures of overall disease activity. Arthritis Rheum. 2004;50:3418–3426. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
