

Prevalence of and risk factors for postoperative pulmonary complications after lung cancer surgery in patients with early-stage COPD
- PMID: 27366059
- PMCID: PMC4914071
- DOI: 10.2147/COPD.S105206
Prevalence of and risk factors for postoperative pulmonary complications after lung cancer surgery in patients with early-stage COPD
Abstract
Purpose: This study aimed to investigate whether the prevalence of postoperative pulmonary complications (PPCs) in patients with non-small-cell lung cancer (NSCLC) is even higher in the early stages of COPD than in such patients with normal lung function and to verify the usefulness of symptom- or quality of life (QoL)-based scores in predicting risk for PPCs.
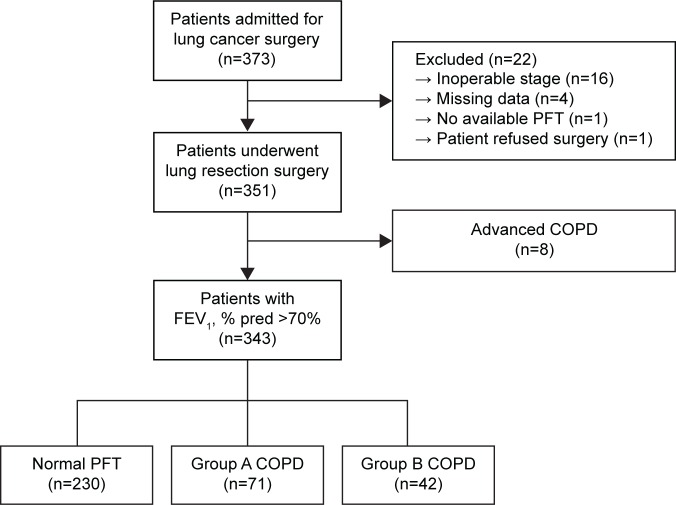
Patients and methods: Patients undergoing pulmonary resection for NSCLC between July 2012 and October 2014 were prospectively enrolled. Preoperative measurements of lung function, dyspnea, and QoL, operative characteristics, PPCs, duration of postoperative hospitalization, and in-hospital mortality were assessed.
Results: Among 351 consecutive patients with NSCLC, 343 patients with forced expiratory volume in 1 second (FEV1) ≥70% of predicted value were enrolled. At least one PPC occurred in 57 (16.6%) patients. Prevalence of PPC was higher in patients with COPD (30.1%) than in those with normal spirometry (10.0%; P<0.001). However, in patients with COPD, the prevalence of PPC was not different in patients with FEV1 ≥70% compared to those with FEV1 <70% and between group A (low risk and less symptoms) and group B (low risk and more symptoms) patients with COPD, based on the new Global initiative for chronic Obstructive Lung Disease 2011 guidelines. In patients with COPD, body mass index (odds ratio [OR]: 0.80, P=0.007), carbon monoxide diffusing capacity of the lung (DLCO), % predicted value (OR: 0.97, P=0.024), and operation time (OR: 1.01, P=0.003), but not COPD assessment test or St George Respiratory Questionnaire scores, were significantly associated with PPCs.
Conclusion: Even in patients with early-stage COPD, the prevalence of PPCs is higher than in patients with NSCLC with normal spirometry. However, this rate is not different between group A and group B patients with COPD. In accordance with this, scores based on symptoms or QoL are not predictors of risk of PPCs in patients with early-stage COPD.
Keywords: early COPD; postoperative pulmonary complication; prevalence; risk factor.
Figures
References
-
- Wang J, Olak J, Ultmann RE, Ferguson MK. Assessment of pulmonary complications after lung resection. Ann Thorac Surg. 1999;67(5):1444–1447. - PubMed
-
- Hazelrigg SR, Landreneau RJ, Boley TM, et al. The effect of muscle-sparing versus standard posterolateral thoracotomy on pulmonary function, muscle strength, and postoperative pain. J Thorac Cardiovasc Surg. 1991;101(3):394–400. discussion 400–401. - PubMed
-
- Busch E, Verazin G, Antkowiak JG, Driscoll D, Takita H. Pulmonary complications in patients undergoing thoracotomy for lung carcinoma. Chest. 1994;105(3):760–766. - PubMed
-
- Bolliger CT, Jordan P, Soler M, et al. Exercise capacity as a predictor of postoperative complications in lung resection candidates. Am J Respir Crit Care Med. 1995;151(5):1472–1480. - PubMed
-
- Epstein SK, Faling LJ, Daly BD, Celli BR. Inability to perform bicycle ergometry predicts increased morbidity and mortality after lung resection. Chest. 1995;107(2):311–316. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
