

The pattern of prognostic and risk indicators among women with breast cancer undergoing modified radical mastectomy in Dar es Salaam, Tanzania
- PMID: 27366204
- PMCID: PMC4928319
- DOI: 10.1186/s13027-016-0075-8
The pattern of prognostic and risk indicators among women with breast cancer undergoing modified radical mastectomy in Dar es Salaam, Tanzania
Abstract
Background: Breast cancer is the commonest female malignancy globally and the second (after uterine cervix) in sub-Saharan Africa including Tanzania. Prognostic indicators reportedly influence post-mastectomy adjuvant therapy by predicting risks on survival and recurrence although in Tanzania this data is lacking. Here, we evaluate the pattern of prognostic and risk indicators among women with breast cancer undergoing modified-radical-mastectomy (MRM) at Muhimbili National Hospital (MNH) and Tumaini Hospital (TH), Dar es Salaam, Tanzania.
Methods: This hospital-based prospective cross-sectional study included female patients undergoing MRM from April 2011 to January 2012. Clinical stage I-III patients were enrolled after being scheduled for mastectomy. Patients with evidence of distant metastasis (stage IV) were excluded. Mastectomy and axillary lymph nodes biopsies were submitted to the Histopathology laboratory for grade, type, nodal and margins status. Data was collected using a structured questionnaire and analyzed using SPSS.
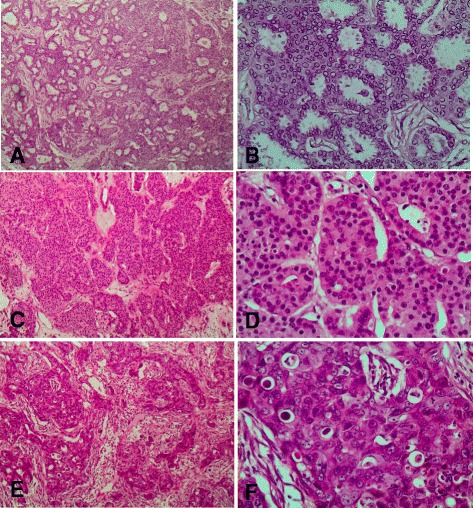
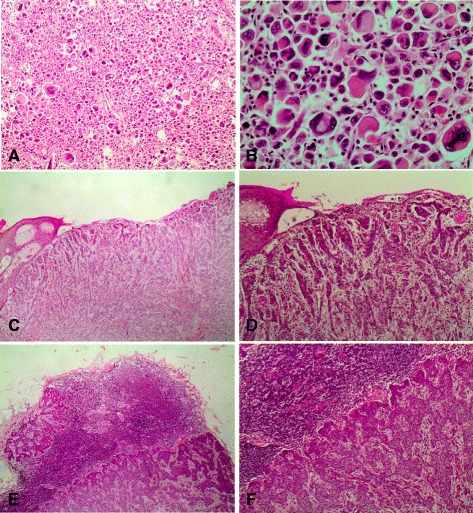
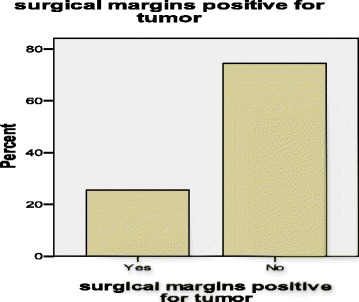
Results: A total of 348 patients were admitted with breast cancer including 86 patients (with 16 from TH having similar demography and presentation) meeting inclusion criteria. Age-range at diagnosis was 28-79 years, mean 52.1 years. Most (89 %) attained menarche after 11 years. About 56 % were postmenopausal. The majority (78 %) were multiparous with positive family history in 14.1 and 37.6 % used hormonal contraceptives. About 27.1 % were social alcohol drinkers. The majority (61 %) had T4b disease, 75.6 % had positive axillary nodes including 42.7 % with 4-9 involved nodes (N2). The commonest (91.9 %) histological type was invasive ductal carcinoma. Lobular, medullary and mucinous carcinomas were rare. Most (83.7 %) of our patients presented with stage III and the rest stage II. Intermediate- and high-grade tumors accounted for 73.5 %. Following MRM, 25 % of our patients had positive surgical margins and similarly for the base.
Conclusions: Most of our breast cancer patients present with frequent risks including younger age, multiparity, hormonal contraceptives use, alcohol use and family history. Unfavourable prognostic indicators including late stages, large primary tumor size, skin infiltration, positive surgical margins, positive axillary lymph nodes and a high histological grade were associated. A sustainable screening program by self-examination to allow early diagnosis is needed to reduce morbidity and mortality from this cancer.
Figures
Similar articles
-
Characterization of hormonal receptors and human epidermal growth factor receptor-2 in tissues of women with breast cancer at Muhimbili National Hospital, Dar es salaam, Tanzania.Infect Agent Cancer. 2017 Nov 6;12:60. doi: 10.1186/s13027-017-0170-5. eCollection 2017. Infect Agent Cancer. 2017. PMID: 29142588 Free PMC article.
-
Local recurrences and distant metastases after breast-conserving surgery and radiation therapy for early breast cancer.Int J Radiat Oncol Biol Phys. 1999 Jan 1;43(1):25-38. doi: 10.1016/s0360-3016(98)00365-4. Int J Radiat Oncol Biol Phys. 1999. PMID: 9989511
-
Long-term follow-up of axillary node-positive breast cancer patients receiving adjuvant systemic therapy alone: patterns of recurrence.Int J Radiat Oncol Biol Phys. 1997 Jun 1;38(3):541-50. doi: 10.1016/s0360-3016(97)00001-1. Int J Radiat Oncol Biol Phys. 1997. PMID: 9231678
-
Overview of resistance to systemic therapy in patients with breast cancer.Adv Exp Med Biol. 2007;608:1-22. doi: 10.1007/978-0-387-74039-3_1. Adv Exp Med Biol. 2007. PMID: 17993229 Review.
-
The role of radiotherapy in patients undergoing mastectomy for carcinoma of the breast.Clin Oncol (R Coll Radiol). 2000;12(3):158-65. doi: 10.1053/clon.2000.9143. Clin Oncol (R Coll Radiol). 2000. PMID: 10942332 Review.
Cited by
-
Educational Opportunities for Down-Staging Breast Cancer in Low-Income Countries: an Example from Tanzania.J Cancer Educ. 2019 Dec;34(6):1225-1230. doi: 10.1007/s13187-019-01587-2. J Cancer Educ. 2019. PMID: 31435911
-
Characterization of hormonal receptors and human epidermal growth factor receptor-2 in tissues of women with breast cancer at Muhimbili National Hospital, Dar es salaam, Tanzania.Infect Agent Cancer. 2017 Nov 6;12:60. doi: 10.1186/s13027-017-0170-5. eCollection 2017. Infect Agent Cancer. 2017. PMID: 29142588 Free PMC article.
-
Predictors of breast cancer screening among women of reproductive age in Tanzania: Evidence from DHS 2022.PLoS One. 2024 Nov 1;19(11):e0298996. doi: 10.1371/journal.pone.0298996. eCollection 2024. PLoS One. 2024. PMID: 39485789 Free PMC article.
-
The role of clinical breast examination and fine needle aspiration cytology in early detection of breast cancer: A cross-sectional study nested in a cohort in a low-resource setting.Womens Health (Lond). 2024 Jan-Dec;20:17455057241250131. doi: 10.1177/17455057241250131. Womens Health (Lond). 2024. PMID: 38725253 Free PMC article.
-
Delayed diagnostic evaluation of symptomatic breast cancer in sub-Saharan Africa: A qualitative study of Tanzanian women.PLoS One. 2022 Oct 6;17(10):e0275639. doi: 10.1371/journal.pone.0275639. eCollection 2022. PLoS One. 2022. PMID: 36201503 Free PMC article.
References
-
- Amir H, Kitinya JN, Parkin DM. A comparative study of carcinoma of the breast in an African population. East Afr Med J. 1994;71(4):215–218. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
