

Endoscopic management of cerebrospinal fluid rhinorrhea
- PMID: 27366243
- PMCID: PMC4849285
- DOI: 10.4103/1793-5482.145101
Endoscopic management of cerebrospinal fluid rhinorrhea
Abstract
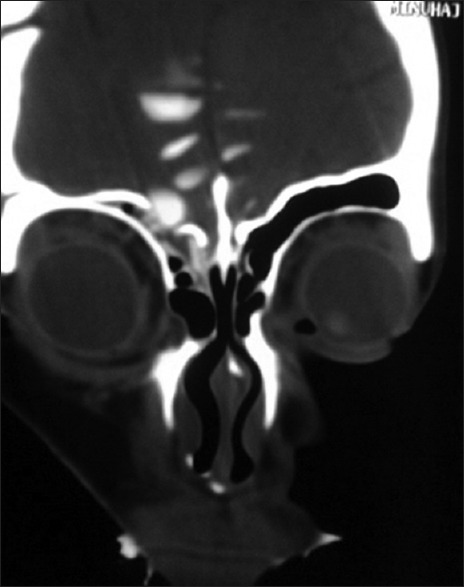
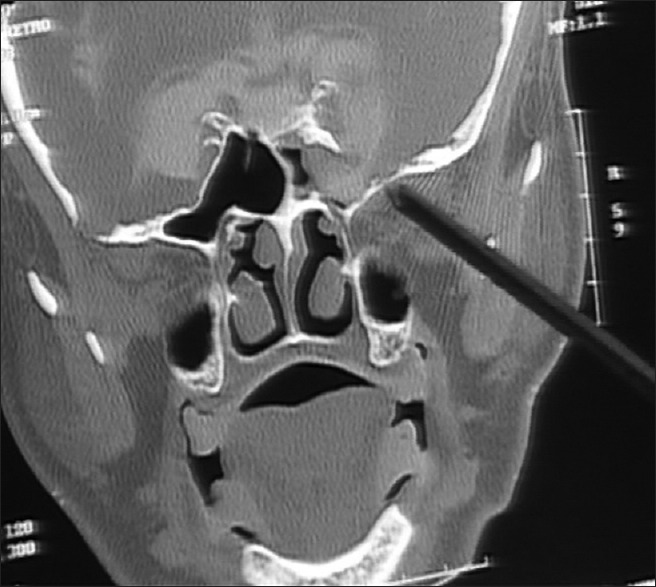
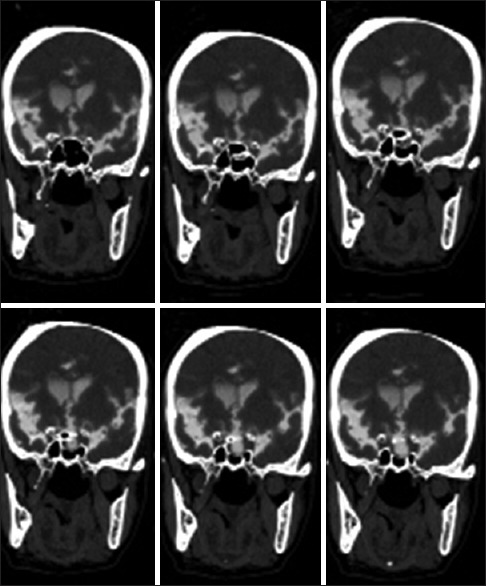
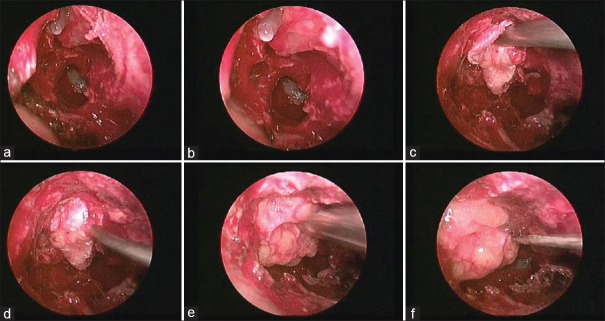
Cerebrospinal fluid (CSF) rhinorrhea occurs due to communication between the intracranial subarachnoid space and the sinonasal mucosa. It could be due to trauma, raised intracranial pressure (ICP), tumors, erosive diseases, and congenital skull defects. Some leaks could be spontaneous without any specific etiology. The potential leak sites include the cribriform plate, ethmoid, sphenoid, and frontal sinus. Glucose estimation, although non-specific, is the most popular and readily available method of diagnosis. Glucose concentration of > 30 mg/dl without any blood contamination strongly suggests presence and the absence of glucose rules out CSF in the fluid. Beta-2 transferrin test confirms the diagnosis. High-resolution computed tomography and magnetic resonance cisternography are complementary to each other and are the investigation of choice. Surgical intervention is indicated, when conservative management fails to prevent risk of meningitis. Endoscopic closure has revolutionized the management of CSF rhinorrhea due to its less morbidity and better closure rate. It is usually best suited for small defects in cribriform plate, sphenoid, and ethmoid sinus. Large defects can be repaired when sufficient experience is acquired. Most frontal sinus leaks, although difficult, can be successfully closed by modified Lothrop procedure. Factors associated with increased recurrences are middle age, obese female, raised ICP, diabetes mellitus, lateral sphenoid leaks, superior and lateral extension in frontal sinus, multiple leaks, and extensive skull base defects. Appropriate treatment for raised ICP, in addition to proper repair, should be done to prevent recurrence. Long follow-up is required before leveling successful repair as recurrences may occur very late.
Keywords: Cerebrospinal fluid pressure; cerebrospinal fluid; cerebrospinal fluid rhinorrhea; endoscopic surgical procedure; skull base.
Conflict of interest statement
Figures

References
-
- Yadav YR, Shenoy R, Mukerji G, Parihar V. Water jet dissection technique for endoscopic third ventriculostomy minimises the risk of bleeding and neurological complications in obstructive hydrocephalus with a thick and opaque third ventricle floor. Minim Invasive Neurosurg. 2010;53:155–8. - PubMed
-
- Yadav YR, Parihar V, Sinha M, Jain N. Endoscopic treatment of supra sellar arachnoid cyst. Neurol India. 2010;58:280–83. - PubMed
-
- Landeiro JA, Lázaro B, Melo MH. Endonasal endoscopicrepair of cerebrospinal fluid rhinorrhea. Minim Invasive Neurosurg. 2004;47:173–7. - PubMed
-
- Yadav YR, Parihar V, Agarwal M, Sherekar S, Bhatele PR. Endoscopic vascular decompression of the trigeminal nerve. Minim Invasive Neurosurg. 2011;54:110–4. - PubMed
-
- Yadav YR, Yadav S, Sherekar S, Parihar V. A new minimally invasive tubular brain retractor system for surgery of deep intracerebral hematoma. Neurol India. 2011;59:74–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources