

Effects of Esmolol on the Prevention of Haemodynamic Responses to Tracheal Extubation after Craniotomy Operations
- PMID: 27366396
- PMCID: PMC4894164
- DOI: 10.5152/TJAR.2013.57
Effects of Esmolol on the Prevention of Haemodynamic Responses to Tracheal Extubation after Craniotomy Operations
Abstract
Objective: The aim of this study was to evaluate the effects of esmolol infusion on the prevention of haemodynamic responses to tracheal extubation in patients undergoing elective craniotomy.
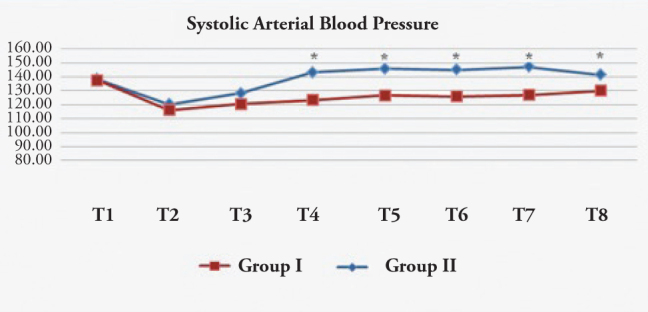
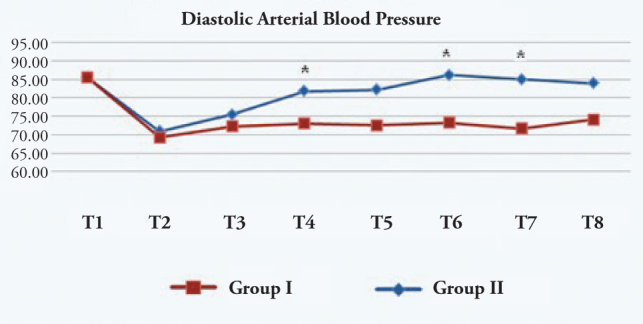
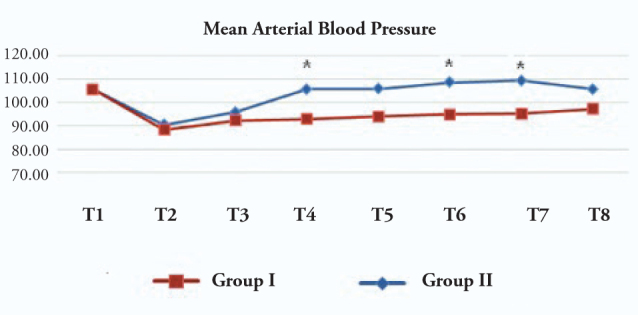
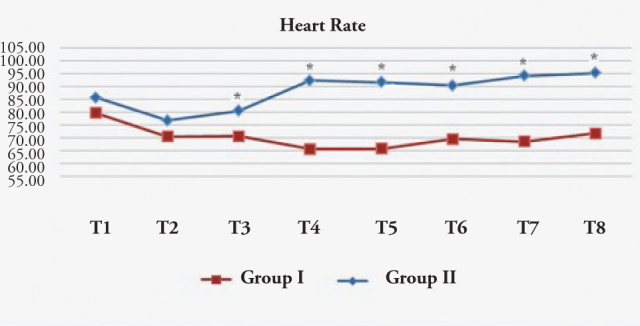
Methods: With approval from the Medical School Ethics Committee at Marmara University and the patients' written consent, 30 patients between 20-65 years of age undergoing elective craniotomy were randomly placed in either the Group Esmolol (n=15) or the Group Control (n=15). Anaesthesia was induced with 5-7 mg kg(-1) thiopental sodium, 1 μg kg(-1) remifentanil, and 0.1 mg kg(-1) vecuronium bromide iv, and was maintained with 1 MAC sevoflurane in oxygen-air mixture (50:50) and 0.25 μg kg(-1) min(-1) remifentanil infusion. At the end of the operation, patients inhaled 100% oxygen after the discontinuation of the anaesthetic agents. For Group Esmolol, 5 min before extubation 2 mg kg(-1) esmolol in 50 mL was infused over 10 min (0.2 μg kg(-1) min(-1)), while for Group Control, 50 mL saline was infused over 10 min. The quality of extubation was evaluated with a 5 point scale, recording heat rate, systolic, diastolic, and mean arterial pressures before infusion, 1 min after infusion, during extubation, and at 1, 3, 5, and 10 min after extubation.
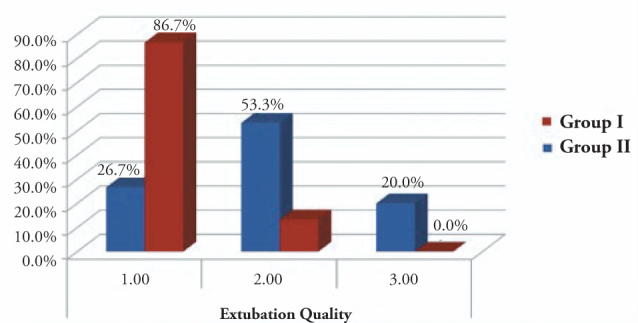
Results: In the esmolol group, systolic, diastolic, and mean arterial pressures, as well as heart rate, decreased significantly after esmolol infusion and were significantly lower than in the control group after extubation (p<0.05). The ratio of patients with an extubation score of one was significantly higher in the esmolol group than in the control group (p<0.05).
Conclusion: We concluded that 2 mg kg(-1) esmolol infusion before extubation can prevent hypertension and tachycardia caused by extubation in patients undergoing elective craniotomy.
Keywords: Craniotomy; esmolol; extubation.
Figures
References
-
- Sulaiman S, Karthekeyan RB, Vakamudi M, Sundar AS, Ravullapalli H, Gandham R. The effects of dexmedetomidine on attenuation of stress response to endotracheal intubation in patients undergoing elective off-pump coronary artery bypass grafting. Ann Card Anaesth. 2012;15:39–43. - PubMed
-
- Akhlagh SH, Vaziri MT, Masoumi T, Anbardan SJ. Hemodynamic response to tracheal intubation via direct laryngoscopy and intubating laryngeal mask airway (ILMA) in patients undergoing coronary artery bypass graft (CABG) Middle East J Anesthesiol. 2011;21:99–103. - PubMed
-
- Marek W, Muckenhoff K, Prabhakar NR. Significance of pulmonary vagal afferents for respiratory muscle activity in the cat. J Physiol Pharmacol. 2008;59:407–20. - PubMed
-
- Siddiqui N, Katznelson R, Friedman Z. Heart rate/blood pressure response and airway morbidity following tracheal intubation with direct laryngoscopy, GlideScope and Trachlight: a randomized control trial. Eur J Anaesthesiol. 2009;26:740–5. - PubMed
-
- Kayhan Z, Aldemir D, Mutlu H, Oğüş E. Which is responsible for the haemodynamic response due to laryngoscopy and endotracheal intubation? Catecholamines, vasopressin or angiotensin? Eur J Anaesthesiol. 2005;22:780–5. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous