

Total Magnetic Resonance Imaging Burden of Small Vessel Disease in Cerebral Amyloid Angiopathy: An Imaging-Pathologic Study of Concept Validation
- PMID: 27366898
- PMCID: PMC5283697
- DOI: 10.1001/jamaneurol.2016.0832
Total Magnetic Resonance Imaging Burden of Small Vessel Disease in Cerebral Amyloid Angiopathy: An Imaging-Pathologic Study of Concept Validation
Abstract
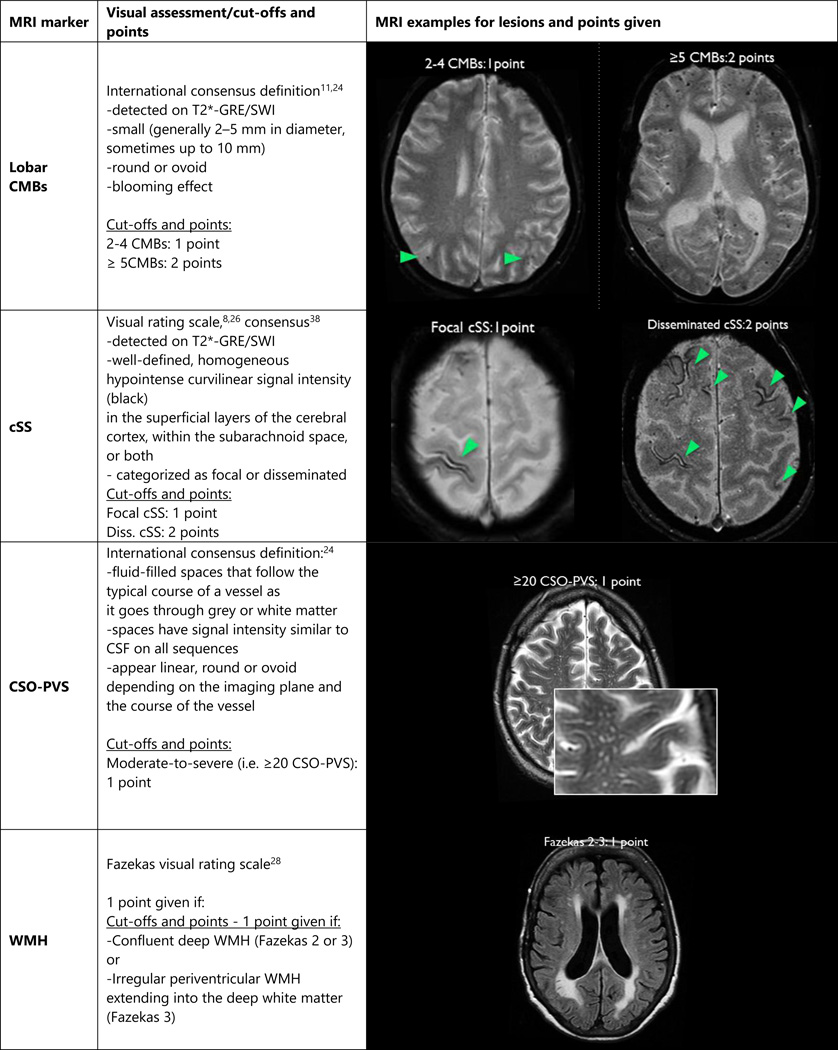
Importance: Cerebral amyloid angiopathy (CAA) is characteristically associated with magnetic resonance imaging (MRI) biomarkers of small vessel brain injury, including strictly lobar cerebral microbleeds, cortical superficial siderosis, centrum semiovale perivascular spaces, and white matter hyperintensities. Although these neuroimaging markers reflect distinct pathophysiologic aspects in CAA, no studies to date have combined these structural imaging features to gauge total brain small vessel disease burden in CAA.
Objectives: To investigate whether a composite score can be developed to capture the total brain MRI burden of small vessel disease in CAA and to explore whether this score contributes independent and complementary information about CAA severity, defined as intracerebral hemorrhage during life or bleeding-related neuropathologic changes.
Design, setting, and participants: This retrospective, cross-sectional study examined a single-center neuropathologic CAA cohort of eligible patients from the Massachusetts General Hospital from January 1, 1997, through December 31, 2012. Data analysis was performed from January 2, 2015, to January 9, 2016. Patients with pathologic evidence of CAA (ie, any presence of CAA from routinely collected brain biopsy specimen, biopsy specimen at hematoma evacuation, or autopsy) and available brain MRI sequences of adequate quality, including T2-weighted, T2*-weighted gradient-recalled echo, and/or susceptibility-weighted imaging and fluid-attenuated inversion recovery sequences, were considered for the study.
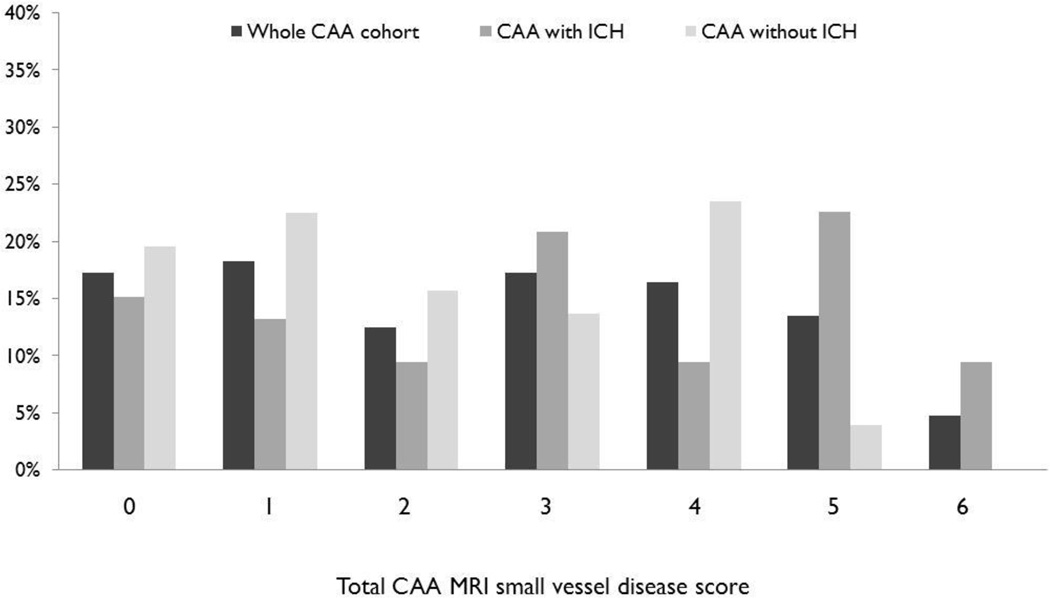
Main outcomes and measures: Brain MRIs were rated for lobar cerebral microbleeds, cortical superficial siderosis, centrum semiovale perivascular spaces, and white matter hyperintensities. All 4 MRI lesions were incorporated into a prespecified ordinal total small vessel disease score, ranging from 0 to 6 points. Associations with severity of CAA-associated vasculopathic changes (fibrinoid necrosis and concentric splitting of the wall), clinical presentation, number of intracerebral hemorrhages, and other imaging markers not included in the score were explored using logistic and ordinal regression.
Results: In total, 105 patients with pathologically defined CAA were included: 52 with autopsies, 22 with brain biopsy specimens, and 31 with pathologic samples from hematoma evacuations. The mean (range) age of the patients was 73 (71-74) years, and 55 (52.4%) were women. In multivariable ordinal regression analysis, severity of CAA-associated vasculopathic changes (odds ratio, 2.40; 95% CI, 1.06-5.45; P = .04) and CAA presentation with symptomatic intracerebral hemorrhage (odds ratio, 2.23; 95% CI, 1.07-4.64; P = .03) were independently associated with the total MRI small vessel disease score. The score was associated with small, acute, diffusion-weighted imaging lesions and posterior white matter hyperintensities in adjusted analyses.
Conclusions and relevance: This study provides evidence of concept validity of a total MRI small vessel disease score in CAA. After further validation, this approach can be potentially used in prospective clinical studies.
Figures
References
-
- Charidimou A, Gang Q, Werring DJ. Sporadic cerebral amyloid angiopathy revisited: recent insights into pathophysiology and clinical spectrum. J Neurol Neurosurg Psychiatry. 2012 Feb;83(2):124–137. - PubMed
-
- Vinters HV. Cerebral amyloid angiopathy. A critical review. Stroke. 1987 Mar-Apr;18(2):311–324. - PubMed
-
- Mandybur TI. Cerebral amyloid angiopathy: the vascular pathology and complications. J Neuropathol Exp Neurol. 1986 Jan;45(1):79–90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
