

Changing HIV treatment eligibility under health system constraints in sub-Saharan Africa: investment needs, population health gains, and cost-effectiveness
- PMID: 27367487
- PMCID: PMC5017264
- DOI: 10.1097/QAD.0000000000001190
Changing HIV treatment eligibility under health system constraints in sub-Saharan Africa: investment needs, population health gains, and cost-effectiveness
Abstract
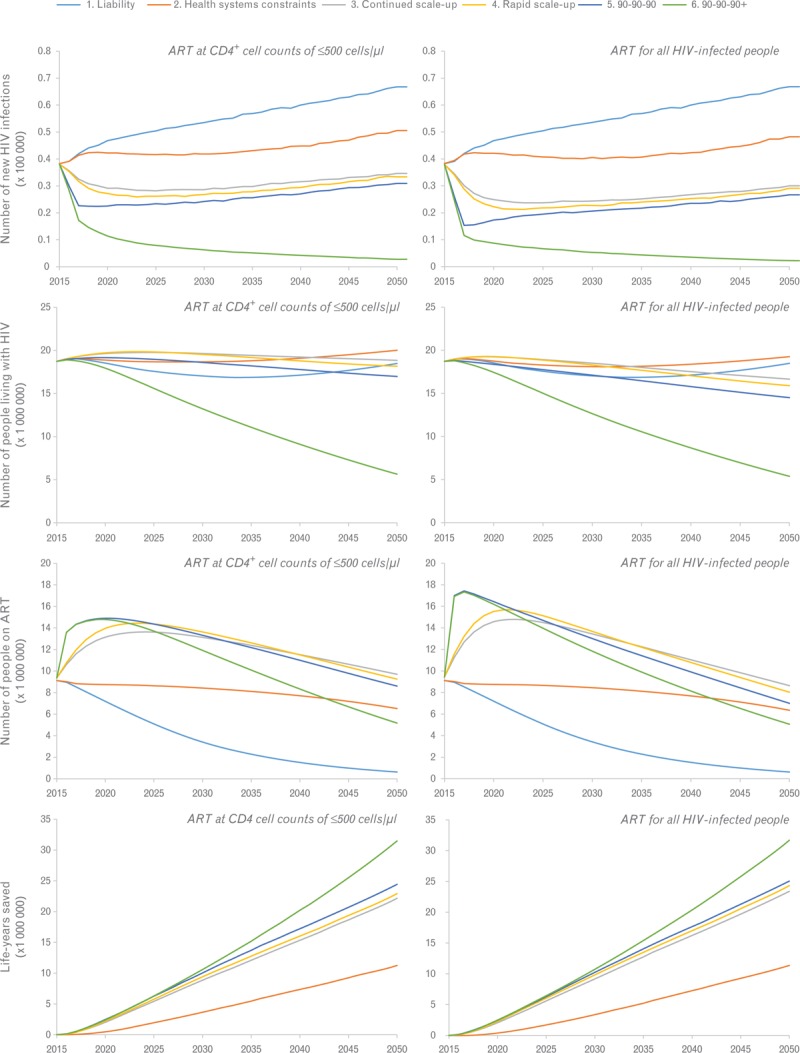
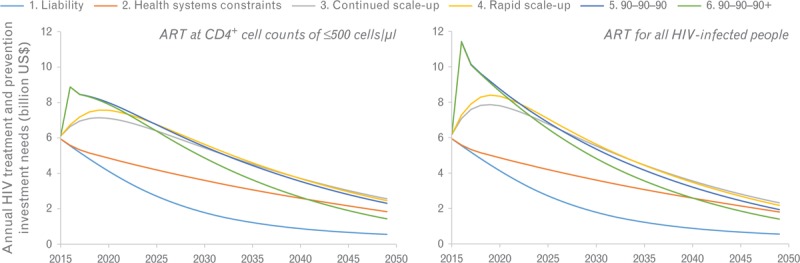
Objective: We estimated the investment needs, population health gains, and cost-effectiveness of different policy options for scaling-up prevention and treatment of HIV in the 10 countries that currently comprise 80% of all people living with HIV in sub-Saharan Africa (Ethiopia, Kenya, Malawi, Mozambique, Nigeria, South Africa, Tanzania, Uganda, Zambia, and Zimbabwe).
Design: We adapted the established STDSIM model to capture the health system dynamics: demand-side and supply-side constraints in the delivery of antiretroviral treatment (ART).
Methods: We compared different scenarios of supply-side (i.e. health system capacity) and demand-side (i.e. health seeking behavior) constraints, and determined the impact of changing guidelines to ART eligibility at any CD4 cell count within these constraints.
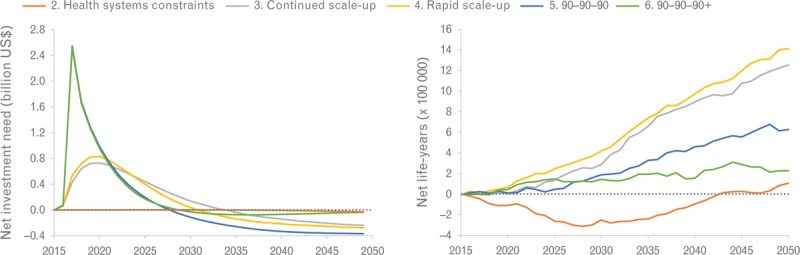
Results: Continuing current scale-up would require US$178 billion by 2050. Changing guidelines to ART at any CD4 cell count is cost-effective under all constraints tested in the model, especially in demand-side constrained health systems because earlier initiation prevents loss-to-follow-up of patients not yet eligible. Changing guidelines under current demand-side constraints would avert 1.8 million infections at US$208 per life-year saved.
Conclusion: Treatment eligibility at any CD4 cell count would be cost-effective, even under health system constraints. Excessive loss-to-follow-up and mortality in patients not eligible for treatment can be avoided by changing guidelines in demand-side constrained systems. The financial obligation for sustaining the AIDS response in sub-Saharan Africa over the next 35 years is substantial and requires strong, long-term commitment of policy-makers and donors to continue to allocate substantial parts of their budgets.
Figures
References
-
- UNAIDS. Report on the global AIDS epidemic 2015. Geneva: UNAIDS; 2015.
-
- Govindasamy D, Ford N, Kranzer K. Risk factors, barriers and facilitators for linkage to antiretroviral therapy care: a systematic review. AIDS 2012; 26:2059–2067. - PubMed
-
- UNAIDS. AIDSinfo Online Database. http://aidsinfoonline.org/devinfo/libraries/aspx/Home.aspx [Accessed 1 August 2015].
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
