

Simple risk factors to predict urgent endoscopy in nonvariceal upper gastrointestinal bleeding pre-endoscopically
- PMID: 27367977
- PMCID: PMC4937891
- DOI: 10.1097/MD.0000000000003603
Simple risk factors to predict urgent endoscopy in nonvariceal upper gastrointestinal bleeding pre-endoscopically
Abstract
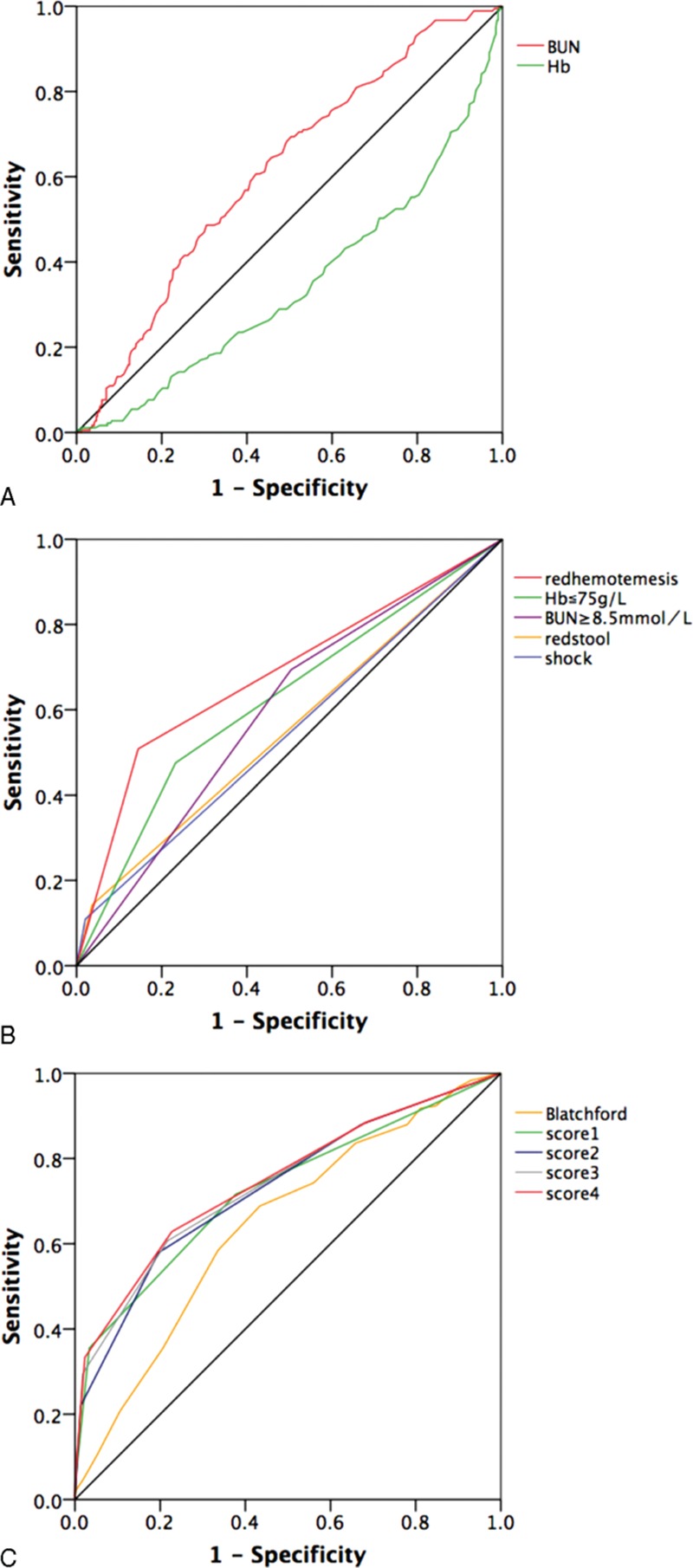
The goal of this study is to evaluate how to predict high-risk nonvariceal upper gastrointestinal bleeding (NVUGIB) pre-endoscopically. A total of 569 NVUGIB patients between Match 2011 and January 2015 were retrospectively studied. The clinical characteristics and laboratory data were statistically analyzed. The severity of NVUGIB was based on high-risk NVUGIB (Forrest I-IIb), and low-risk NVUGIB (Forrest IIc and III). By logistic regression and receiver-operating characteristic curve, simple risk score systems were derived which predicted patients' risks of potentially needing endoscopic intervention to control bleeding. Risk score systems combined of patients' serum hemoglobin (Hb) ≤75 g/L, red hematemesis, red stool, shock, and blood urine nitrogen ≥8.5 mmol/L within 24 hours after admission were derived. As for each one of these clinical signs, the relatively high specificity was 97.9% for shock, 96.4% for red stool, 85.5% for red hematemesis, 76.7% for Hb ≤75 g/L, and the sensitivity was 50.8% for red hematemesis, 47.5% for Hb ≤75 g/L, 14.2% for red stool, and 10.9% for shock. When these 5 clinical signs were presented as a risk score system, the highest area of receiver-operating characteristic curve was 0.746, with sensitivity 0.675 and specificity 0.733, which discriminated well with high-risk NVUGIB. These simple risk factors identified patients with high-risk NVUGIB of needing treatment to manage their bleeding pre-endoscopically. Further validation in the clinic was required.
Conflict of interest statement
The authors declared that there was no funding/conflict of interest in this retrospective study.
Figures
References
-
- Meier R, Wettstein AR. Treatment of acute nonvariceal upper gastrointestinal hemorrhage. Digestion 1999; 60 suppl 2:47–52. - PubMed
-
- Zhaoshen Li YD, Xianbao Zhan. The guideline about the diagnosis and treatment of acute nonvariceal upper gastrointestinal bleeding (2009, Hangzhou). Chin J Dig Endosc 2009; 26:449–452.
-
- Sung JJ, Chan FK, Chen M, et al. Asia-Pacific Working Group consensus on non-variceal upper gastrointestinal bleeding. Gut 2011; 60:1170–1177. - PubMed
-
- Physicians CCoE. Consensus on the emergency treatment and treatment of acute upper gastrointestinal bleeding. Chin J Crit Care Med 2015; 35:961–970.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
