

Intraoperative portal vein insulin assay combined with occlusion of the pancreas for complex pancreatogenous hypoglycemia: Two cases report
- PMID: 27367988
- PMCID: PMC4937902
- DOI: 10.1097/MD.0000000000003928
Intraoperative portal vein insulin assay combined with occlusion of the pancreas for complex pancreatogenous hypoglycemia: Two cases report
Abstract
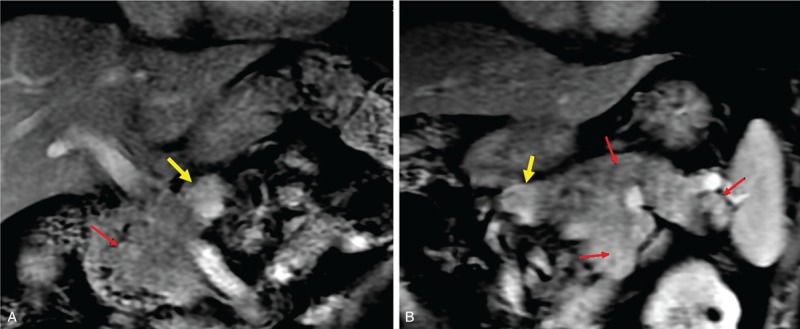
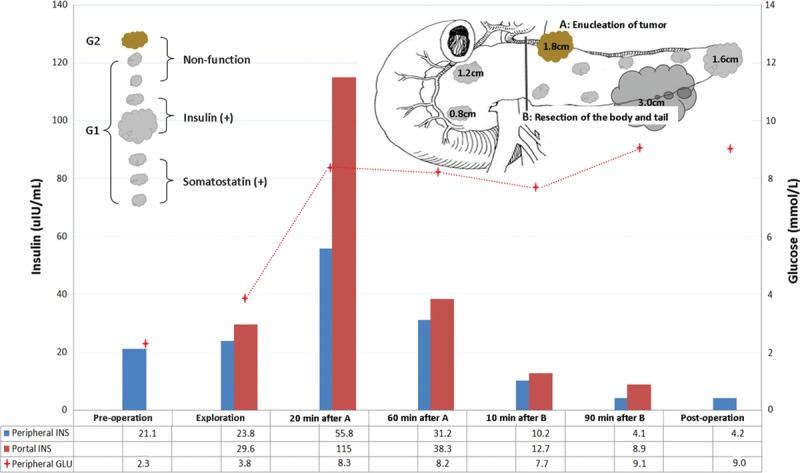
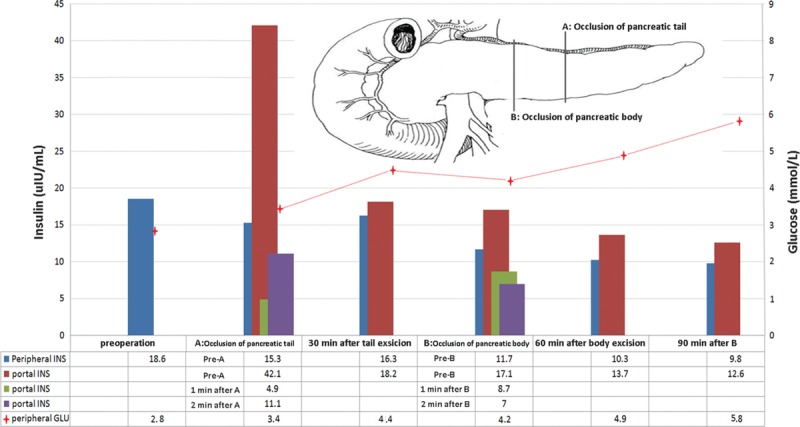
Intraoperative localization and confirmation of complete resection of the hypersecreting tissue are the 2 main challenges in the management of pancreatogenous hypoglycemia. Here, we report our experience with intraoperative portal vein insulin assay combined with occlusion of the pancreas in the management of pancreatogenous hypoglycemia. Clinical courses of 2 patients with biochemical evidence of a pancreatogenous hypoglycemia were studied. The preoperative diagnosis was multiple endocrine neoplasia 1 (MEN-1) and nesidioblastosis, respectively. Rapid intraoperative portal vein insulin assay combined with occlusion of the pancreas was used to localize and confirm complete excision of the hypersecreting tissue. Hypoglycemia was successfully treated in both the patients. In the MEN-1 patient, 2 small tumors in the head of pancreas were not resected, as they were deemed noninsulin secreting by intraoperative portal vein insulin assay, thus avoiding a total pancreatectomy. In the patient with nesidioblastosis, using intraoperative portal vein insulin assay combined with occlusion of the pancreas, an appropriate amount of pancreatic tissue was resected thereby avoiding recurrence and diabetes. This technique may be of particular value in patients with complex conditions such as MEN-1 and nesidioblastosis, to localize and achieve complete resection of hypersecreting pancreatic tissue.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Tutt GO, Edis AJ, Service FJ, et al. Plasma glucose monitoring during operation for insulinoma: a critical reappraisal. Surgery 1980; 88:351–356. - PubMed
-
- Katz LB, Aufses AH, Jr, Rayfield E, et al. Preoperative localisation and intraoperative glucose monitoring in the management of patients with pancreatic insulinoma. Surg Gynecol Obstet 1986; 163:509–512. - PubMed
-
- Yao CZ, Zeng XJ, Niu ZP. Rapid assay of insulin in portosplenic blood for insulinoma. Chin Med J 1984; 97:57–60. - PubMed
-
- Proye C, Pattou F, Carnaille B, et al. Intraoperative insulin measurement during surgical management of insulinomas. World J Surg 1998; 22:1218–1224. - PubMed
-
- Scott-Coombes D, Eatock F, Henley R, et al. Use of intraoperative insulin assay for the localisation of insulinoma. World J Surg 2009; 33:969–972. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
