

Hepatic resection or transarterial chemoembolization for hepatocellular carcinoma with portal vein tumor thrombus
- PMID: 27367992
- PMCID: PMC4937906
- DOI: 10.1097/MD.0000000000003959
Hepatic resection or transarterial chemoembolization for hepatocellular carcinoma with portal vein tumor thrombus
Abstract
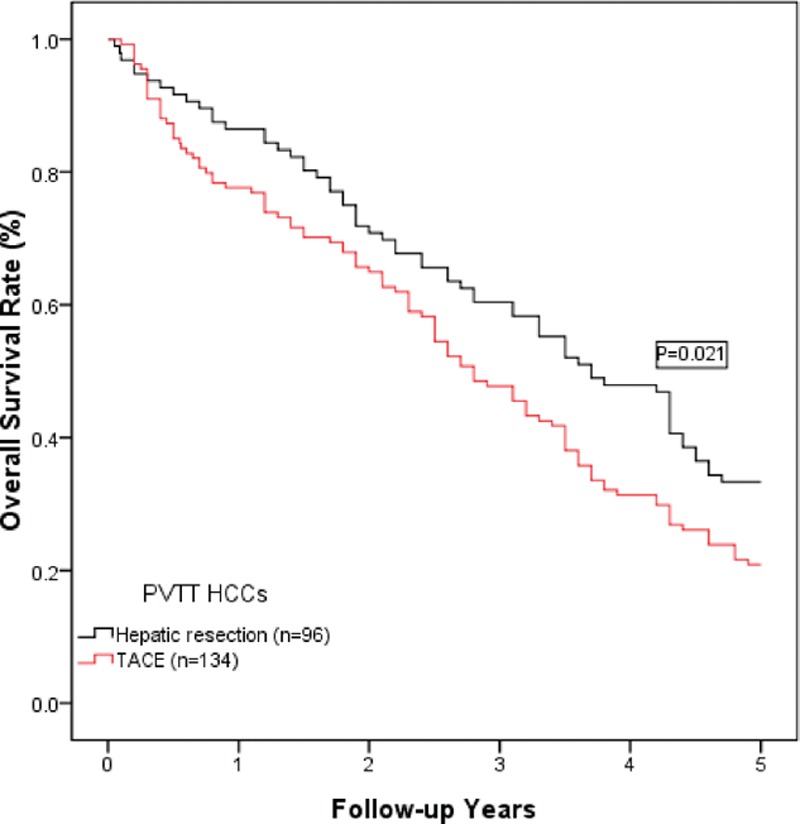
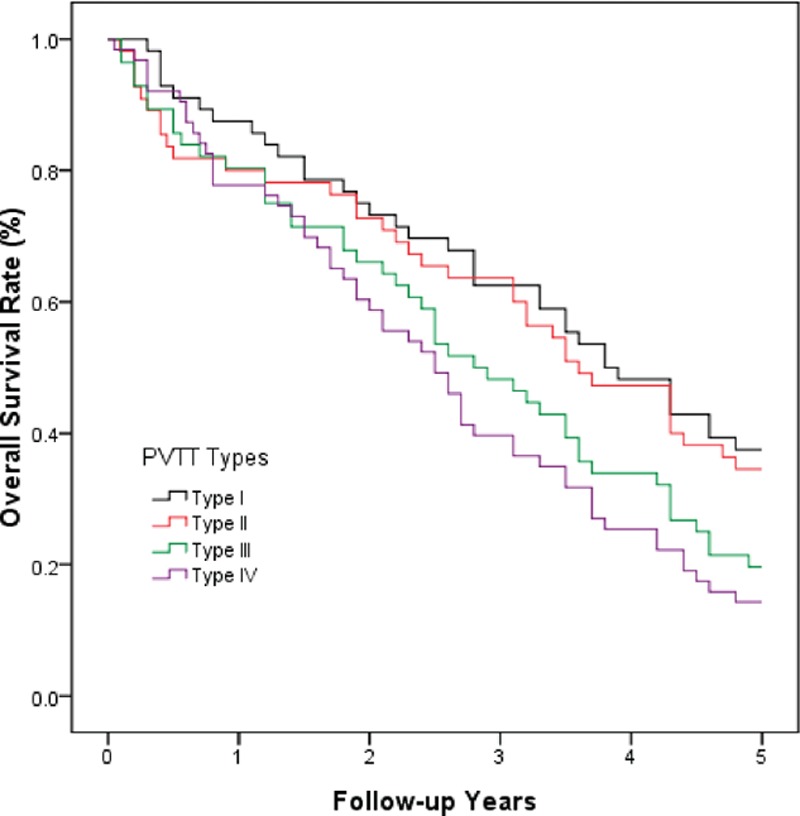
The role of hepatic resection in hepatocellular carcinoma (HCC) with accompanying portal vein tumor thrombus (PVTT) remains controversial. This study aimed to evaluate the surgical outcomes of hepatic resection compared with those of transarterial chemoembolization (TACE) in HCC patients. A retrospective study was conducted using the medical records of 230 HCC patients with portal vein invasion who underwent hepatic resection (96 patients) or TACE (134 patients). The baseline characteristics, tumor characteristics, clinicopathological parameters, and overall survival rates were compared between the 2 groups. The baseline and tumor characteristics were comparable between the hepatic resection and TACE groups. The overall complication rate was 35.4% in the hepatic resection group, which was significantly lower than that in the TACE group (73.0%, P <0.001). However, the serious complication rate (grade ≥3) in the hepatic resection group was 13.5%, which was significantly higher than that in the TACE group (P = 0.003). The cumulative overall survival rates at 1, 3, and 5 years in the hepatic resection group were 86.5%, 60.4%, and 33.3%, respectively. These rates were much higher than those in the TACE group (1-year: 77.6%; 3-year: 47.8%; and 5-year: 20.9%; P = 0.021). The long-term survival was notably better in the patients with types I and II PVTT than in the patients with types III and IV PVTT (P <0.05). The univariate and multivariate analyses indicated that types III and IV PVTT and TACE may have contributed to the poor overall survival following surgery. In HCC patients with PVTT and compensated liver function, hepatic resection is a safe and effective surgical protocol, particularly for patients with type I or II PVTT.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011; 61:69–90. - PubMed
-
- Bosch FX, Ribes J, Diaz M, Cleries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology 2004; 127 (5 suppl 1):S5–S16. - PubMed
-
- Rahbari NN, Mehrabi A, Mollberg NM, et al. Hepatocellular carcinoma: current management and perspectives for the future. Ann Surg 2011; 253:453–469. - PubMed
-
- Peng ZW, Guo RP, Zhang YJ, et al. Hepatic resection versus transcatheter arterial chemoembolization for the treatment of hepatocellular carcinoma with portal vein tumor thrombus. Cancer 2012; 118:4725–4736. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
