

Learning curve for single-incision laparoscopic resection of right-sided colon cancer by complete mesocolic excision
- PMID: 27367999
- PMCID: PMC4937913
- DOI: 10.1097/MD.0000000000003982
Learning curve for single-incision laparoscopic resection of right-sided colon cancer by complete mesocolic excision
Erratum in
-
Erratum: Learning curve for single-incision laparoscopic resection of right-sided colon cancer by complete mesocolic excision: Erratum.Medicine (Baltimore). 2016 Dec 9;95(49):e5662. doi: 10.1097/MD.0000000000005662. eCollection 2016 Dec. Medicine (Baltimore). 2016. PMID: 31265668 Free PMC article.
Abstract
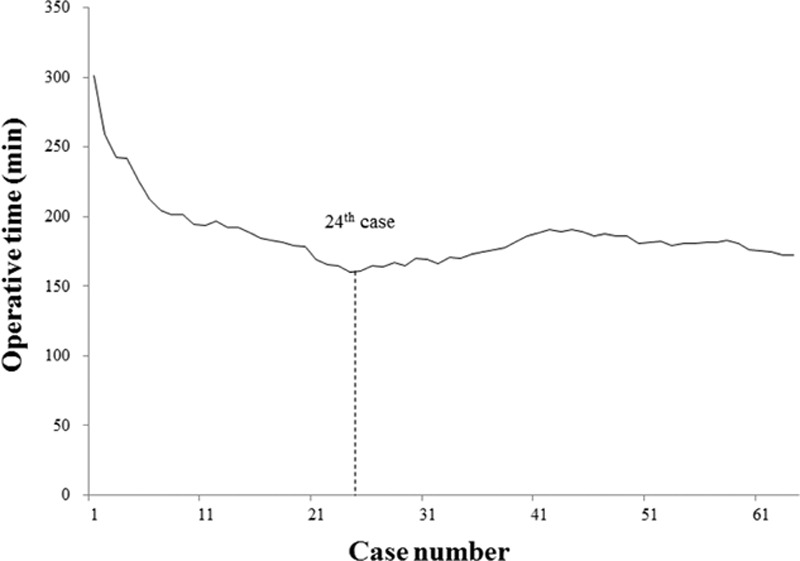
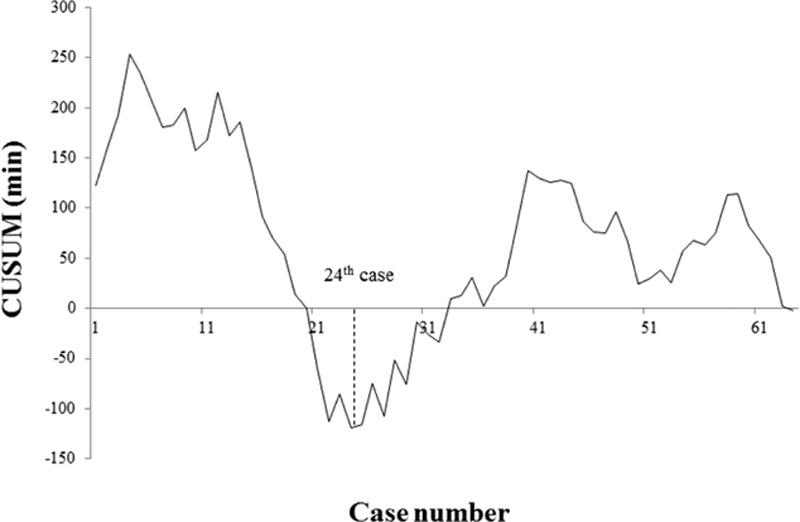
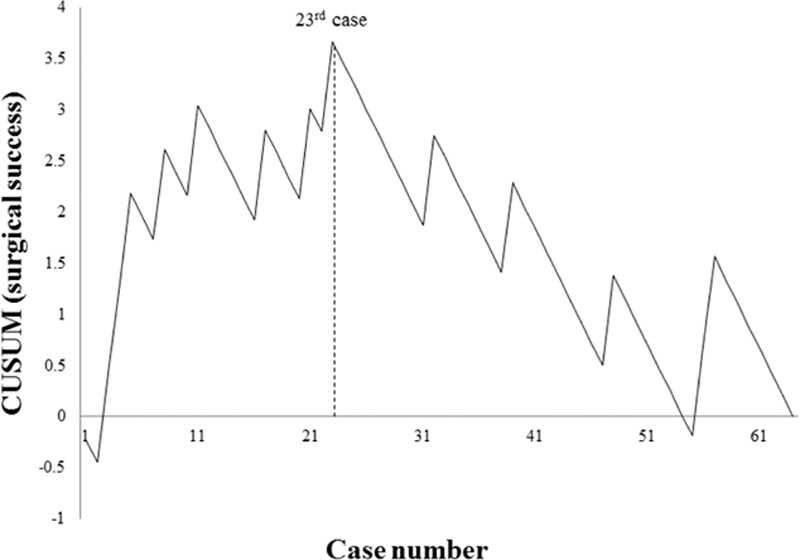
Single-incision laparoscopic surgery is cosmetically beneficial, but technically challenging. In this study, the learning curve (LC) for single-incision laparoscopic right hemicolectomy (SILRC), incorporating complete mesocolic excision to resect right-sided colon cancer, was investigated through multidimensional techniques. Between December 2009 and May 2015, 64 patients each underwent SILRC of right-sided colon cancer at Severance Hospital, performed in all instances by the same surgeon. Moving average and cumulative sum control chart (CUSUM) were used for LC analyses retrospectively. Surgical failure was defined as conversion to conventional laparoscopic surgery, postsurgical morbidity within 30 days, harvested lymph node count <12, or local tumor recurrence. Both moving average and CUSUM graphics of operative time registered nadirs at the 24th patient, with slight ascent thereafter, reaching a plateau at the 40th patient. The CUSUM for surgical success peaked at the 23rd patient. Operative time for 23 patients in phase 1 (1-23) and for 41 patients in phase 2 (24-64) of the LC did not differ significantly. By comparison, significant differences in patients of phase 2 included larger tumor size, higher harvested lymph node counts, longer proximal resection margins, and more advanced disease. As indicated by multidimensional statistical analyses, the LC for SILRC of right-sided colon cancer was 23 patients. In terms of operative time and surgical success, SILRC is feasible for surgeons experienced in LS, but may prove more challenging for novices, given the fundamental technical difficulties of this procedure.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Learning Curve for Single-Incision Laparoscopic Anterior Resection for Sigmoid Colon Cancer.J Am Coll Surg. 2015 Aug;221(2):397-403. doi: 10.1016/j.jamcollsurg.2015.02.016. Epub 2015 Feb 26. J Am Coll Surg. 2015. PMID: 26070396
-
An Optimal Approach for Laparoscopic D3 Lymphadenectomy Plus Complete Mesocolic Excision (D3+CME) for Right-Sided Colon Cancer.Ann Surg Oncol. 2017 May;24(5):1312-1313. doi: 10.1245/s10434-016-5722-1. Epub 2016 Dec 19. Ann Surg Oncol. 2017. PMID: 27995452
-
Learning curve and safety of the implementation of laparoscopic complete mesocolic excision with intracorporeal anastomosis for right-sided colon cancer: results from a propensity score-matched study.Surg Endosc. 2024 Sep;38(9):5114-5121. doi: 10.1007/s00464-024-11086-1. Epub 2024 Jul 19. Surg Endosc. 2024. PMID: 39028345
-
[Mesocolic excision for colonic adenocarcinoma].Bull Cancer. 2017 Feb;104(2):177-181. doi: 10.1016/j.bulcan.2016.11.004. Epub 2016 Nov 29. Bull Cancer. 2017. PMID: 27912892 Review. French.
-
Single-incision right hemicolectomy for malignancy: a feasible technique with standard laparoscopic instrumentation.Colorectal Dis. 2012 Nov;14(11):e764-70. doi: 10.1111/j.1463-1318.2012.03175.x. Colorectal Dis. 2012. PMID: 22776288 Review.
Cited by
-
Definition and reporting of lymphadenectomy and complete mesocolic excision for radical right colectomy: a systematic review.Surg Endosc. 2023 Feb;37(2):846-861. doi: 10.1007/s00464-022-09548-5. Epub 2022 Sep 12. Surg Endosc. 2023. PMID: 36097099 Free PMC article.
-
Resident Learning Curve for Laparoscopic Appendectomy According to Seniority.Ann Coloproctol. 2020 Jul;36(3):163-171. doi: 10.3393/ac.2019.07.20. Epub 2020 Feb 14. Ann Coloproctol. 2020. PMID: 32054238 Free PMC article.
-
Learning curve for single-port robot-assisted colectomy.Ann Coloproctol. 2024 Feb;40(1):44-51. doi: 10.3393/ac.2022.00745.0106. Epub 2022 Dec 20. Ann Coloproctol. 2024. PMID: 36535706 Free PMC article.
-
Erratum: Learning curve for single-incision laparoscopic resection of right-sided colon cancer by complete mesocolic excision: Erratum.Medicine (Baltimore). 2016 Dec 9;95(49):e5662. doi: 10.1097/MD.0000000000005662. eCollection 2016 Dec. Medicine (Baltimore). 2016. PMID: 31265668 Free PMC article.
-
Single-incision laparoscopy surgery: a systematic review.Electron Physician. 2016 Oct 25;8(10):3088-3095. doi: 10.19082/3088. eCollection 2016 Oct. Electron Physician. 2016. PMID: 27957308 Free PMC article. Review.
References
-
- Jayne DG, Thorpe HC, Copeland J, et al. Five-year follow-up of the Medical Research Council CLASICC trial of laparoscopically assisted versus open surgery for colorectal cancer. Br J Surg 2010; 97:1638–1645. - PubMed
-
- Kang SB, Park JW, Jeong SY, et al. Open versus laparoscopic surgery for mid or low rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): short-term outcomes of an open-label randomised controlled trial. Lancet Oncol 2010; 11:637–645. - PubMed
-
- Bagshaw PF, Allardyce RA, Frampton CM, et al. Long-term outcomes of the Australasian randomized clinical trial comparing laparoscopic and conventional open surgical treatments for colon cancer: the Australasian Laparoscopic Colon Cancer Study trial. Ann Surg 2012; 256:915–919. - PubMed
-
- Kadar N, Reich H, Liu CY, et al. Incisional hernias after major laparoscopic gynecologic procedures. Am J Obstet Gynecol 1993; 168:1493–1495. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
