

Severe hyponatremia caused by nab-paclitaxel-induced syndrome of inappropriate antidiuretic hormone secretion: A case report in a patient with metastatic pancreatic adenocarcinoma
- PMID: 27368013
- PMCID: PMC4937927
- DOI: 10.1097/MD.0000000000004006
Severe hyponatremia caused by nab-paclitaxel-induced syndrome of inappropriate antidiuretic hormone secretion: A case report in a patient with metastatic pancreatic adenocarcinoma
Abstract
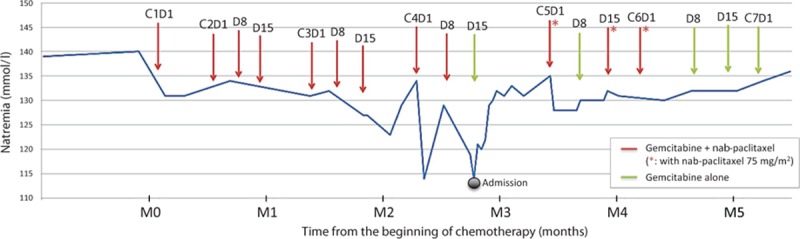
Incidence of pancreatic ductal adenocarcinoma (PDAC) is increasing. Most patients have advanced disease at diagnosis and therapeutic options in this setting are limited. Gemcitabine plus nab-paclitaxel regimen was demonstrated to increase survival compared with gemcitabine monotherapy and is therefore indicated as first-line therapy in patients with metastatic PDAC and performance status Eastern Cooperative Oncology Group (ECOG) 0-2. The safety profile of gemcitabine and nab-paclitaxel combination includes neutropenia, fatigue, and neuropathy as most common adverse events of grade 3 or higher. No case of severe hyponatremia associated with the use of nab-paclitaxel for the treatment of PDAC has been reported to date.We report the case of a 72-year-old Caucasian man with a metastatic PDAC treated with gemcitabine and nab-paclitaxel regimen, who presented with a severe hyponatremia (grade 4) caused by a documented syndrome of inappropriate antidiuretic hormone secretion (SIADH). This SIADH was attributed to nab-paclitaxel after a rigorous imputability analysis, including a rechallenge procedure with dose reduction. After dose and schedule adjustment, nab-paclitaxel was pursued without recurrence of severe hyponatremia and with maintained efficacy.Hyponatremia is a rare but potentially severe complication of nab-paclitaxel therapy that medical oncologists and gastroenterologists should be aware of. Nab-paclitaxel-induced hyponatremia is manageable upon dose and schedule adaptation, and should not contraindicate careful nab-paclitaxel reintroduction. This is of particular interest for a disease in which the therapeutic options are limited.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Rahib L, Smith BD, Aizenberg R, et al. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014; 74:2913–2921. - PubMed
-
- Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma. N Engl J Med 2014; 371:2140–2141. - PubMed
-
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364:1817–1825. - PubMed
-
- Gradishar WJ. Albumin-bound paclitaxel: a next-generation taxane. Expert Opin Pharmacother 2006; 7:1041–1053. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
