

Infective endocarditis in hypertrophic cardiomyopathy: A multicenter, prospective, cohort study
- PMID: 27368014
- PMCID: PMC4937928
- DOI: 10.1097/MD.0000000000004008
Infective endocarditis in hypertrophic cardiomyopathy: A multicenter, prospective, cohort study
Abstract
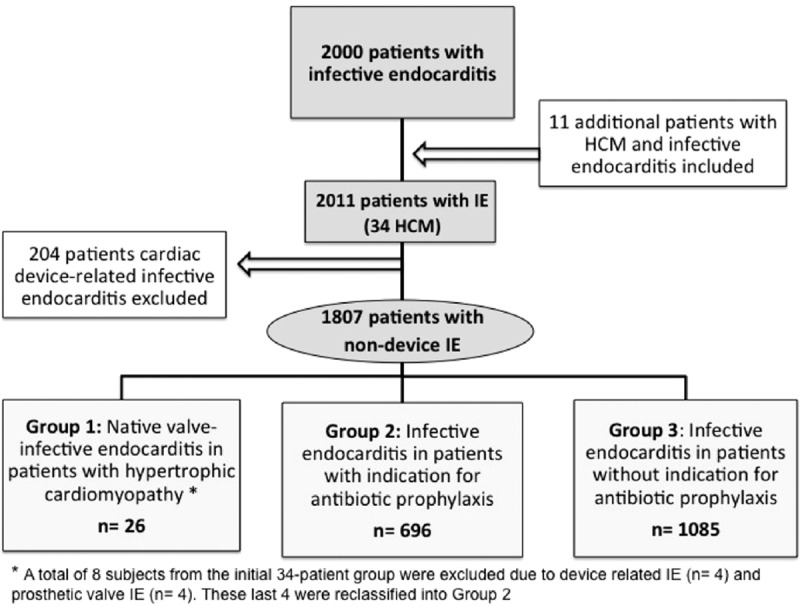
Infective endocarditis (IE) complicating hypertrophic cardiomyopathy (HCM) is a poorly known entity. Although current guidelines do not recommend IE antibiotic prophylaxis (IEAP) in HCM, controversy remains.This study sought to describe the clinical course of a large series of IE HCM and to compare IE in HCM patients with IE patients with and without an indication for IEAP.Data from the GAMES IE registry involving 27 Spanish hospitals were analyzed. From January 2008 to December 2013, 2000 consecutive IE patients were prospectively included in the registry. Eleven IE HCM additional cases from before 2008 were also studied. Clinical, microbiological, and echocardiographic characteristics were analyzed in IE HCM patients (n = 34) and in IE HCM reported in literature (n = 84). Patients with nondevice IE (n = 1807) were classified into 3 groups: group 1, HCM with native-valve IE (n = 26); group 2, patients with IEAP indication (n = 696); group 3, patients with no IEAP indication (n = 1085). IE episode and 1-year follow-up data were gathered.One-year mortality in IE HCM was 42% in our study and 22% in the literature. IE was more frequent, although not exclusive, in obstructive HCM (59% and 74%, respectively). Group 1 exhibited more IE predisposing factors than groups 2 and 3 (62% vs 40% vs 50%, P < 0.01), and more previous dental procedures (23% vs 6% vs 8%, P < 0.01). Furthermore, Group 1 experienced a higher incidence of Streptococcus infections than Group 2 (39% vs 22%, P < 0.01) and similar to Group 3 (39% vs 30%, P = 0.34). Overall mortality was similar among groups (42% vs 36% vs 35%, P = 0.64).IE occurs in HCM patients with and without obstruction. Mortality of IE HCM is high but similar to patients with and without IEAP indication. Predisposing factors, previous dental procedures, and streptococcal infection are higher in IE HCM, suggesting that HCM patients could benefit from IEAP.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Spirito P, Rapezzi C, Bellone P, et al. Infective endocarditis in hypertrophic cardiomyopathy: prevalence, incidence, and indications for antibiotic prophylaxis. Circulation 1999; 99:2132–2137. - PubMed
-
- Alessandri N, Pannarale G, del Monte F, et al. Hypertrophic obstructive cardiomyopathy and infective endocarditis: a report of seven cases and a review of the literature. Eur Heart J 1990; 11:1041–1048. - PubMed
-
- Dajani AS, Taubert KA, Wilson W, et al. Prevention of bacterial endocarditis: recommendations by the American Heart Association. JAMA 1997; 277:1794–1801. - PubMed
-
- Delahaye F, Harbaoui B, Cart-Regal V, et al. Recommendations on prophylaxis for infective endocarditis: dramatic changes over the past seven years. Arch Cardiovasc Dis 2009; 102:233–235. - PubMed
-
- Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation 2007; 116:1736–1754. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
