

Cerebral ischemic events in patients with pancreatic cancer: A retrospective cohort study of 17 patients and a literature review
- PMID: 27368015
- PMCID: PMC4937929
- DOI: 10.1097/MD.0000000000004009
Cerebral ischemic events in patients with pancreatic cancer: A retrospective cohort study of 17 patients and a literature review
Abstract
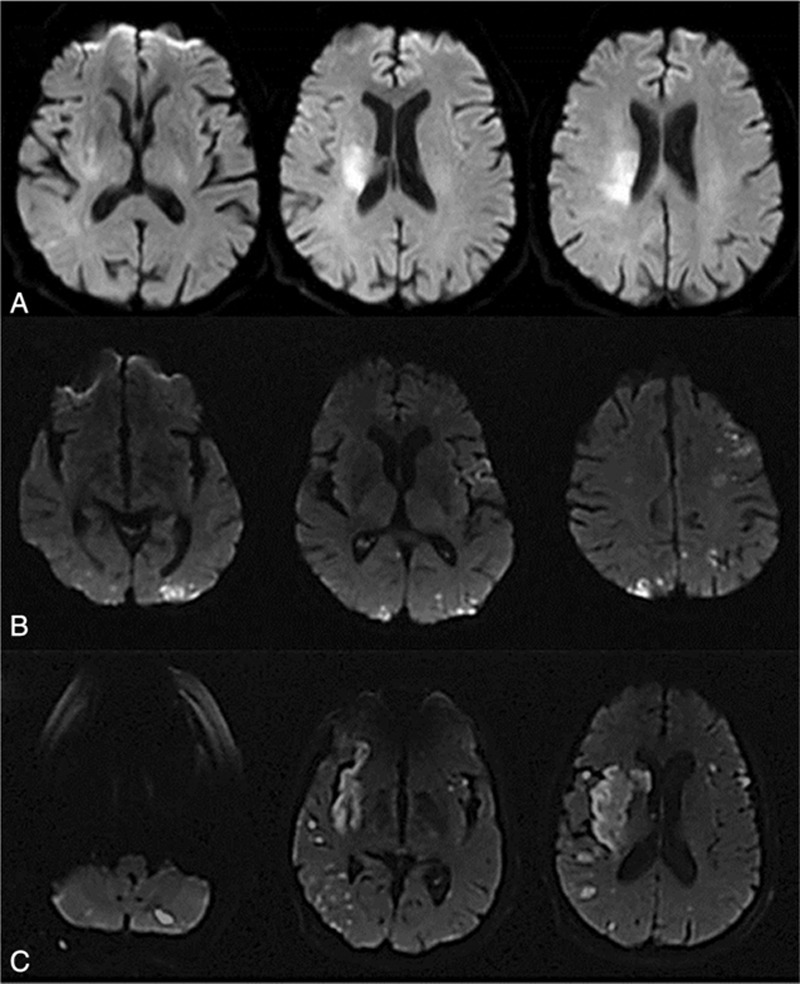
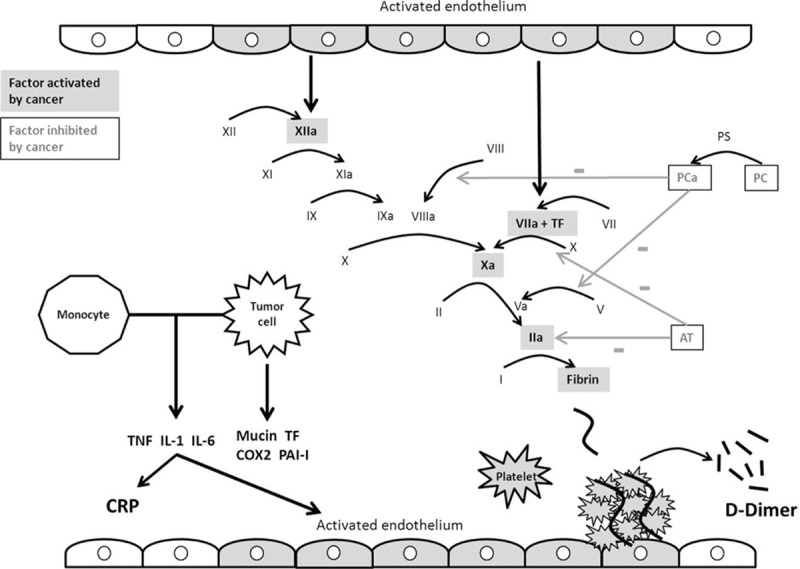
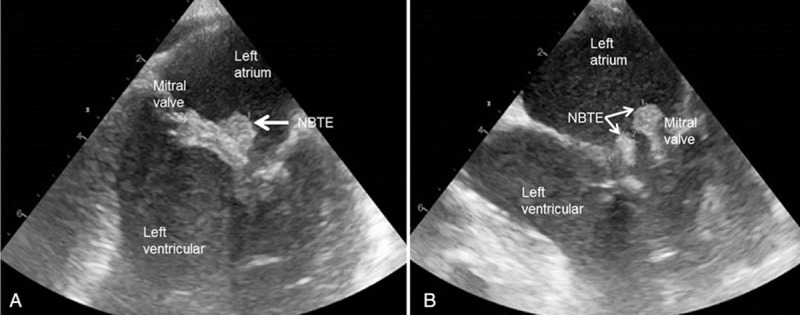
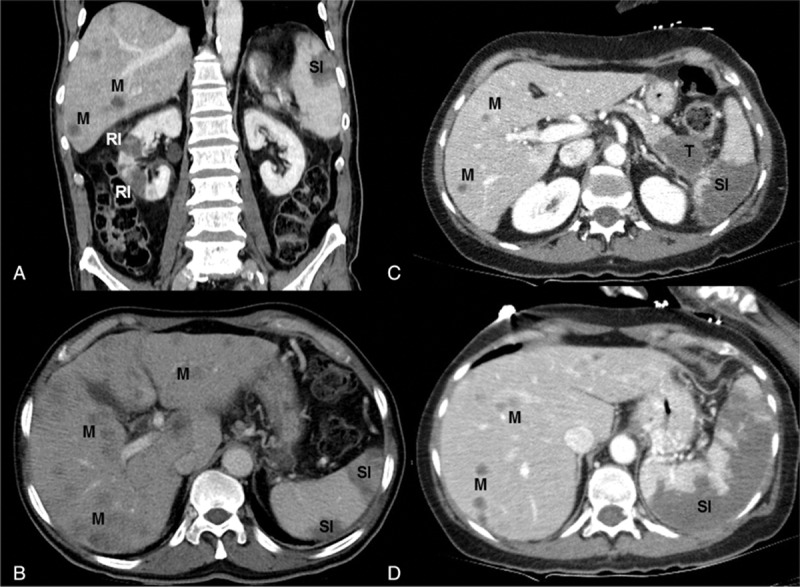
Stroke is a dramatic complication of pancreatic cancer with mechanisms related to oncological disease. A better description of the characteristics of cerebrovascular events would help better understand the pathogeny and protect vulnerable patients. We thus conducted a descriptive analysis of clinical, biological, and radiological features of patients from our centers and literature.We reviewed consecutive cases of patients who presented cerebrovascular events and pancreatic cancer in 4 stroke units in Lorrain (France) between January 1, 2009 and March 31, 2015, and all reported cases of literature. We identified 17 cases in our centers and 18 reported cases. Fifty-seven per cent of patients were male. Median age was 63 ± 14 years and ranged from 23 to 81 years. All cerebral events were ischemic. At the onset of stroke, pancreatic cancer had already been diagnosed in 59% of the patients in our centers for a mean time of 5.4 months. Five of them (29%) were being treated with gemcitabine and 2 (12%) with folfirinox. Adenocarcinoma at metastatic stage was reported in 82% of cases overall. Brain imaging revealed disseminated infarctions in 64%. High median levels of D-dimer (7600 ± 5 × 10 μg/L), C-reactive protein (63 ± 43 mg/L), and elevated prothrombin time (19 ± 6 seconds) were found. Thirty-six per cent of patients explored with echocardiography were diagnosed with nonbacterial thrombotic endocarditis. Ten of our patients received anticoagulant therapy as secondary stroke prevention without any documented recurrence. Nevertheless, outcome was poor with a median survival time of 28 ± 14 days after stroke onset. Cerebral ischemic events occur at advanced stages of pancreatic cancer, most likely by a thromboembolic mechanism. Disseminated infarctions and high D-dimer, C-reactive protein levels, and a high prothrombin time are the most constant characteristics found in this context. All patients should be screened for nonbacterial thrombotic endocarditis as this etiology supports the use of anticoagulant therapy.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Bick RL. Cancer-associated thrombosis. N Engl J Med 2003; 349:109–111. - PubMed
-
- Blom JW, Vanderschoot JP, Oostindiër MJ, et al. Incidence of venous thrombosis in a large cohort of 66,329 cancer patients: results of a record linkage study. J Thromb Haemost 2006; 4:529–535. - PubMed
-
- Epstein AS, Soff GA, Capanu M, et al. Analysis of incidence and clinical outcomes in patients with thromboembolic events and invasive exocrine pancreatic cancer. Cancer 2012; 118:3053–3061. - PubMed
-
- Menapace LA, Peterson DR, Berry A, et al. Symptomatic and incidental thromboembolism are both associated with mortality in pancreatic cancer. Thromb Haemost 2011; 106:371–378. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
