

Immune checkpoint blockade as a potential therapeutic target: surveying CNS malignancies
- PMID: 27370400
- PMCID: PMC5035527
- DOI: 10.1093/neuonc/now132
Immune checkpoint blockade as a potential therapeutic target: surveying CNS malignancies
Abstract
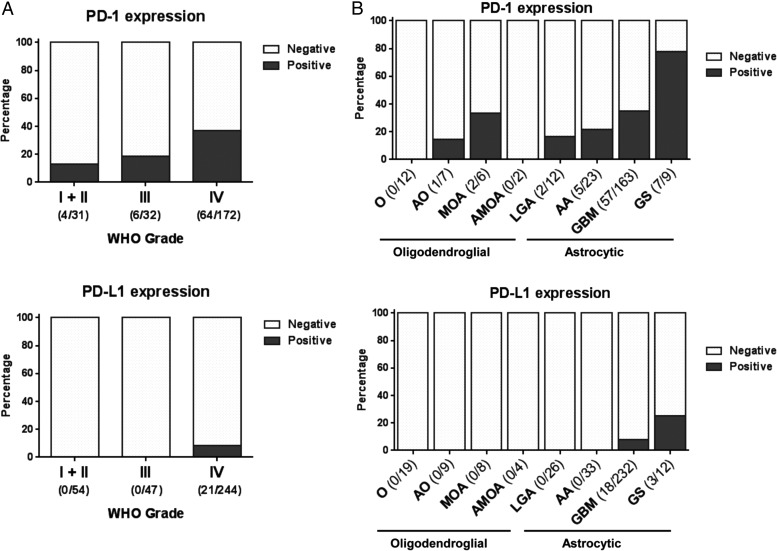
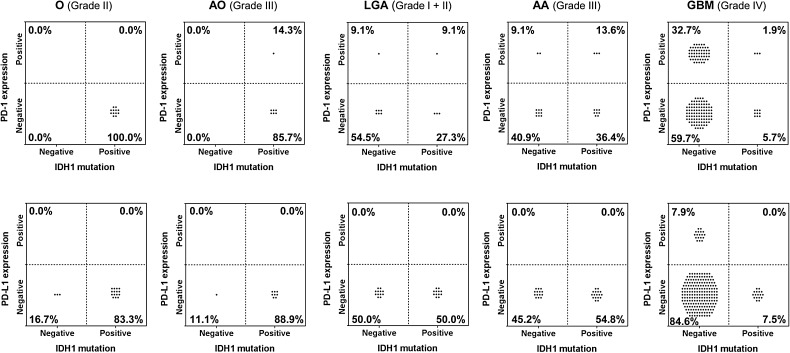
Background: Expression of programmed cell death protein 1 (PD-1)/programmed death ligand 1 (PD-L1) across glioma grades is undocumented, and their interactions with commonly expressed genetic and epigenetic alterations are undefined but nonetheless highly relevant to combinatorial treatments.
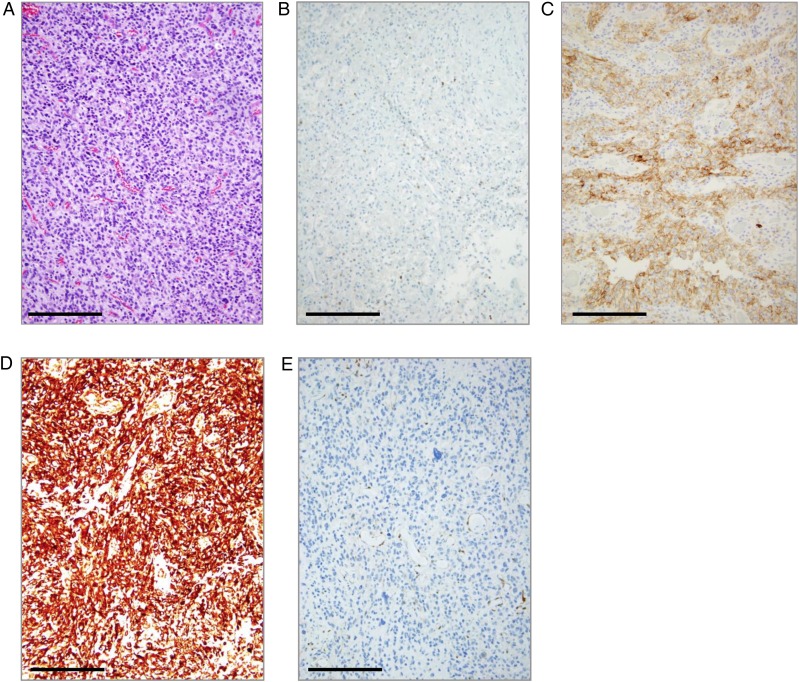
Methods: Patients with CNS malignancies were profiled by Caris Life Sciences from 2009 to 2016. Immunohistochemistry findings for PD-1 on tumor-infiltrating lymphocytes (TIL) and PD-L1 on tumor cells were available for 347 cases. Next-generation sequencing, pyrosequencing, immunohistochemistry, fragment analysis, and fluorescence in situ hybridization were used to determine isocitrate dehydrogenase 1 (IDH1), phosphatase and tensin homolog (PTEN), and tumor protein 53 mutational status, O(6)-DNA methylguanine-methyltransferase promoter methylation (MGMT-Me) status, PTEN expression, plus epidermal growth factor receptor variant III and 1p/19q codeletion status.
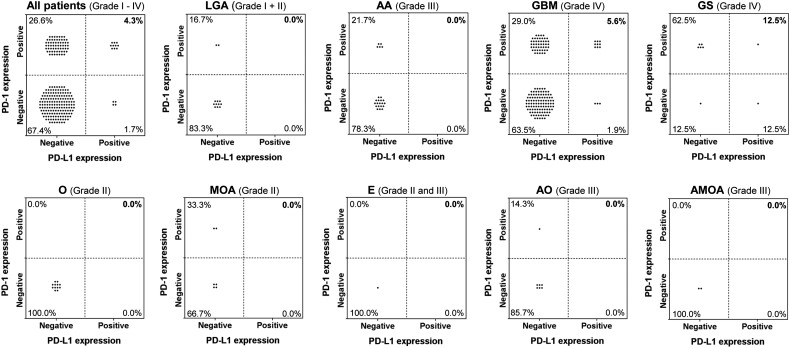
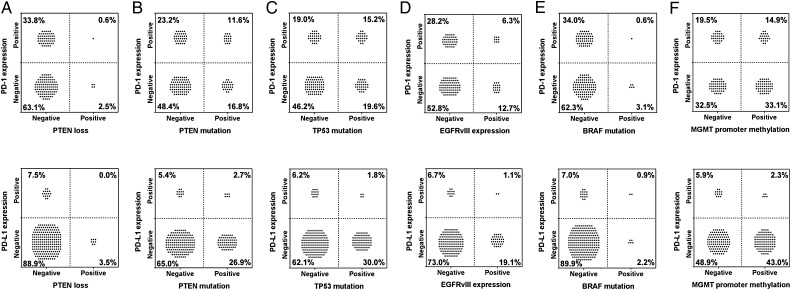
Results: PD-1+ TIL expression and grade IV gliomas were significantly positively correlated (odds ratio [OR]: 6.363; 95% CI: 1.263, 96.236)-especially in gliosarcomas compared with glioblastoma multiforme (P = .014). PD-L1 expression was significantly correlated with tumor grade with all PD-L1+ cases (n = 21) being associated with grade IV gliomas. PD-1+ TIL expression and PD-L1 expression were significantly correlated (OR: 5.209; 95% CI: 1.555, 20.144). Mutations of PTEN, tumor protein 53, BRAF, IDH1, and epidermal growth factor receptor or MGMT-Me did not associate with increased intratumoral expression of either PD-1+ TIL or PD-L1 in glioblastoma multiforme even before false discovery rate correction for multiple comparison.
Conclusions: Targeting immune checkpoints in combination with other therapeutics based on positive biomarker selection will require screening of large patient cohorts.
Keywords: PD-1; PD-L1; glioblastoma; immune checkpoint; low-grade glioma.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
In search of a target: PD-1 and PD-L1 profiling across glioma types.Neuro Oncol. 2016 Oct;18(10):1331-2. doi: 10.1093/neuonc/now162. Epub 2016 Aug 17. Neuro Oncol. 2016. PMID: 27534576 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
