

Different Types of Urinary Steroid Profiling Obtained by High-Performance Liquid Chromatography and Gas Chromatography-Mass Spectrometry in Patients with Adrenocortical Carcinoma
- PMID: 27370636
- PMCID: PMC10355950
- DOI: 10.1007/s12672-016-0267-0
Different Types of Urinary Steroid Profiling Obtained by High-Performance Liquid Chromatography and Gas Chromatography-Mass Spectrometry in Patients with Adrenocortical Carcinoma
Abstract
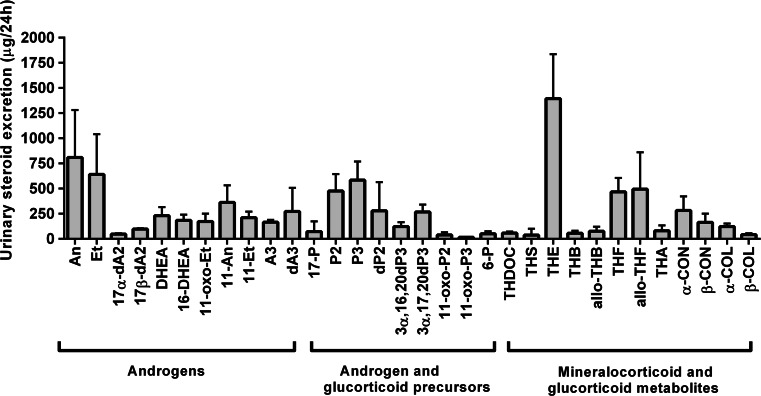
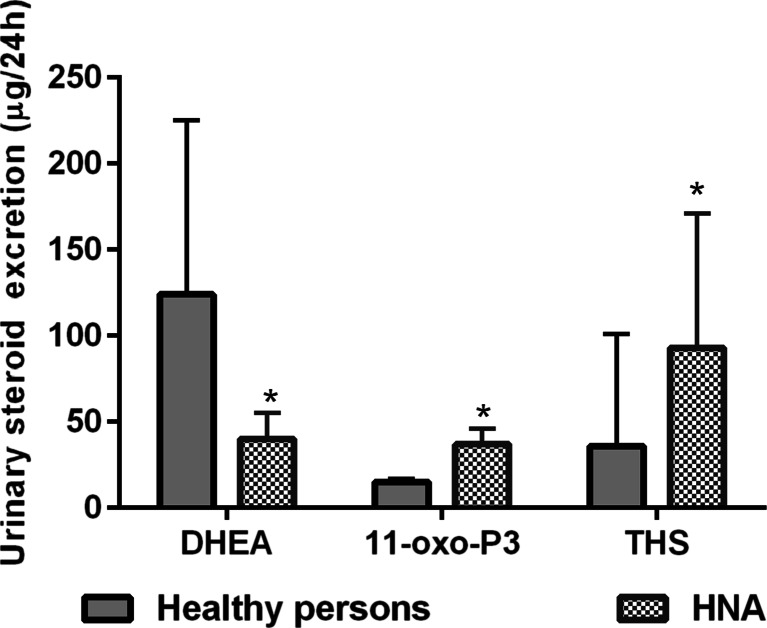
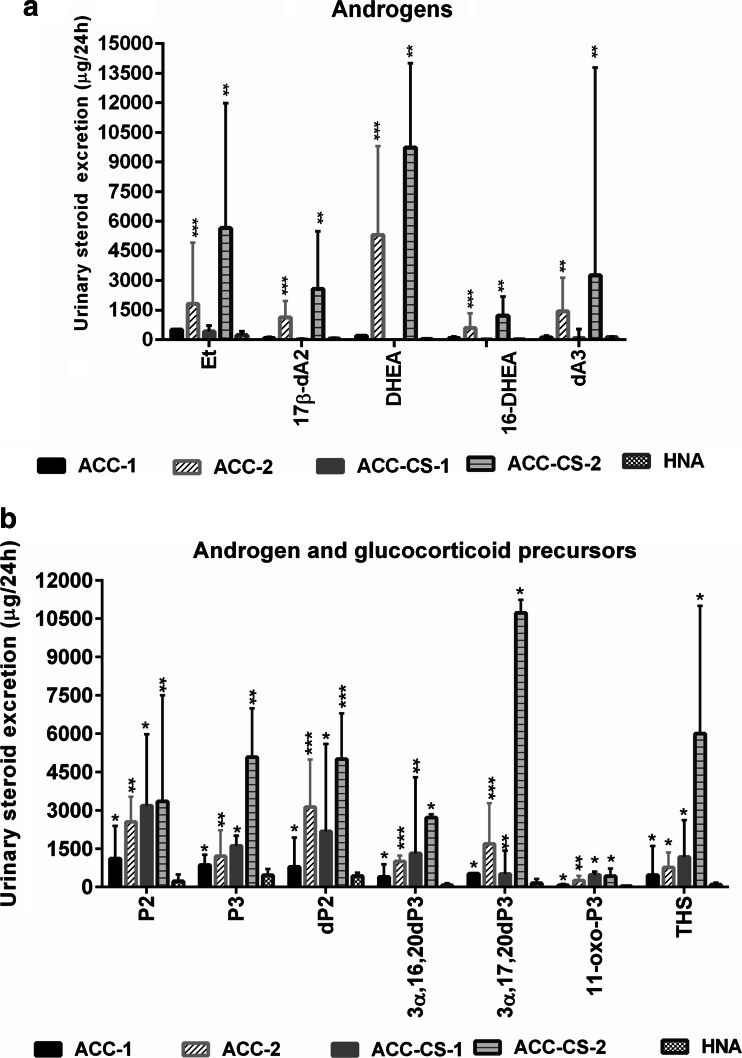
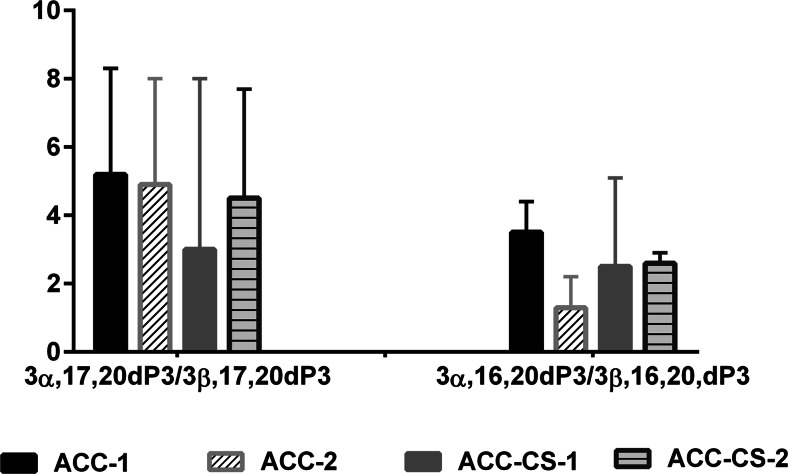
Urinary steroid profiling (USP) was studied using high-performance liquid chromatography (HPLC) and gas chromatography-mass spectrometry (GC-MS) methods in 108 patients with adrenocortical adenoma (ACA) and in 31 patients with adrenocortical carcinoma (ACC). Thirteen ACC and Cushing's syndrome (ACC-CS) patients had two types of USP as well as 18 ACC patients without hypercortisolism. These four types differed by androgen and glucocorticoid secretion of the adrenal cortex. Fifteen main ACC features were observed by GC-MS. Urinary excretion of dehydroepiandrosterone (DHEA) was increased in 67.7 % of ACC patients and tetrahydro-11-deoxycortisol (THS) in 74.2 %. By combination of the following parameters: THS >900 μg/24 h and/or DHEA >1500 μg/24 h with ratios of 3α,16,20-pregnentriol/3β,16,20-pregnentriol (3α,16,20dP3/3β,16,20dP3) less than 6.0 and 3α,17,20dP3/3β,17,20dP3 less than 9.0 and the detection of "non-classical" 5-en-pregnens, not found in ACA and healthy persons, 100 % sensitivity and specificity of ACC and ACA differential diagnosis were achieved. Features of 21-hydroxylase and 11β-hydroxylase deficiency were observed by GC-MS in 32.2 and 61.3 % of the ACC patients, respectively. Additional features for ACC-CS diagnostic were increased urinary excretion of 6β-hydroxycortisol, 18-hydroxycorticosterone, the sum (UFF + UFE) obtained by HPLC, tetrahydrocorticosterone, and the sum (THF + THE + allo-THF) obtained by GC-MS.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Arlt W, Biehl M, Taylor AE, Hahner S, Libé R, Hughes BA, Schneider P, Smith DJ, Stiekema H, Krone N, Porfiri E, Opocher G, Bertherat J, Mantero F, Allolio B, Terzolo M, Nightingale P, Shackleton CH, Bertagna X, Fassnacht M, Stewart PM. Urine steroid metabolomics as a biomarker tool for detecting malignancy in adrenal tumors. J Clin Endocrinol Metab. 2011;96(12):3775–3784. doi: 10.1210/jc.2011-1565. - DOI - PMC - PubMed
-
- Grumbach MM, Biller BM, Braunstein GD, Campbell KK, Carney JA, Godley PA, Harris EL, Lee JK, Oertel YC, Posner MC, Schlechte JA, Wieand HS. Management of the clinically inapparent adrenal mass (“incidentaloma”) Ann Intern Med. 2003;138:424–429. doi: 10.7326/0003-4819-138-5-200303040-00013. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
