

Ventricular stimulus site influences dynamic dispersion of repolarization in the intact human heart
- PMID: 27371682
- PMCID: PMC5142177
- DOI: 10.1152/ajpheart.00159.2016
Ventricular stimulus site influences dynamic dispersion of repolarization in the intact human heart
Abstract
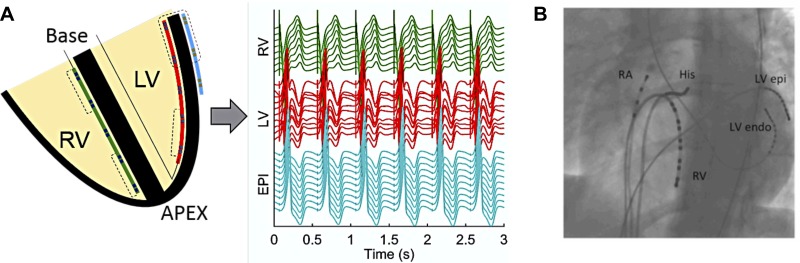
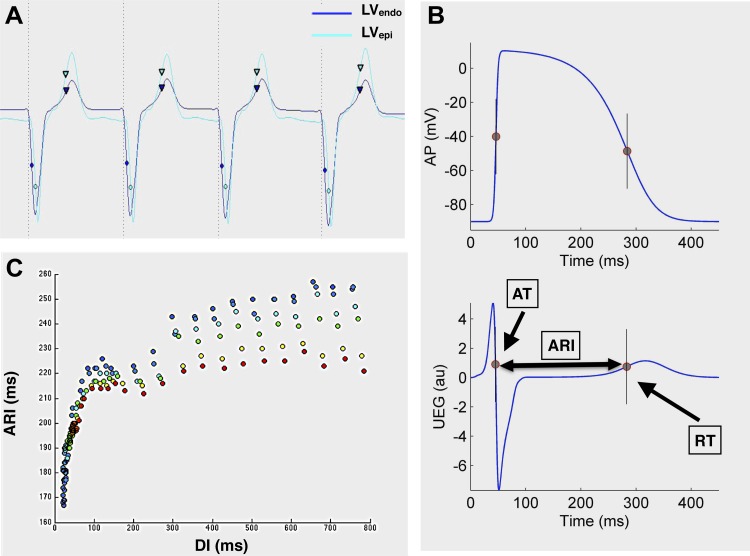
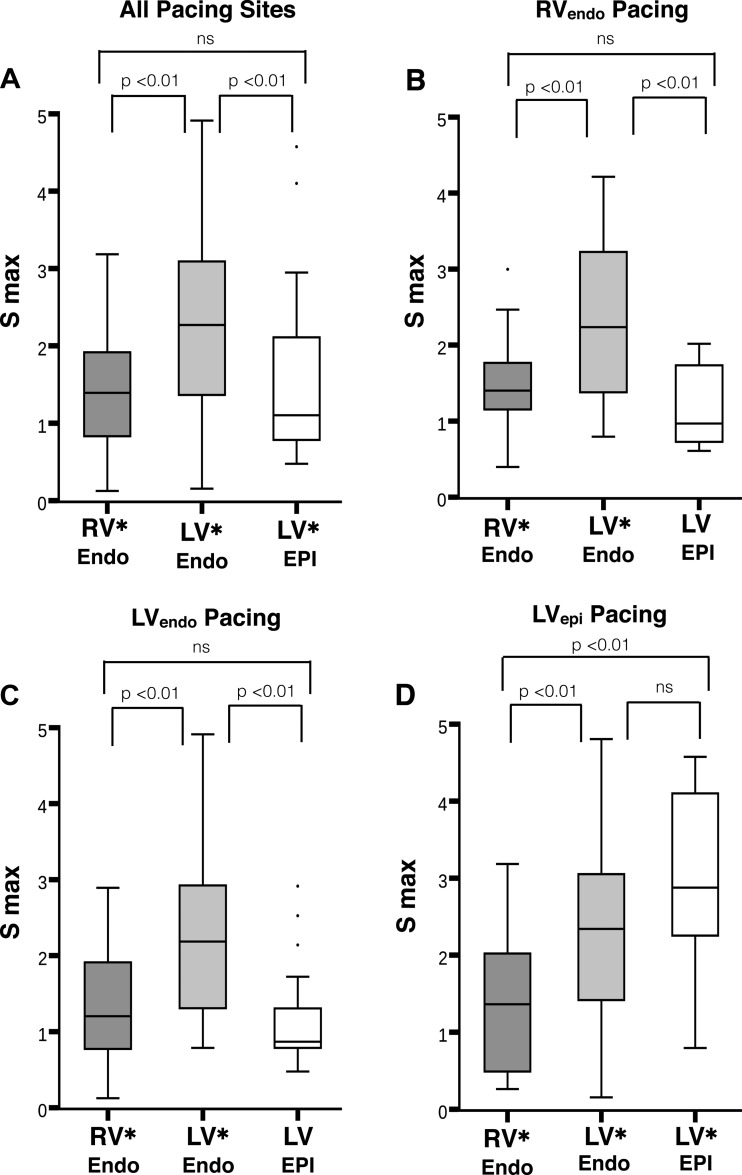
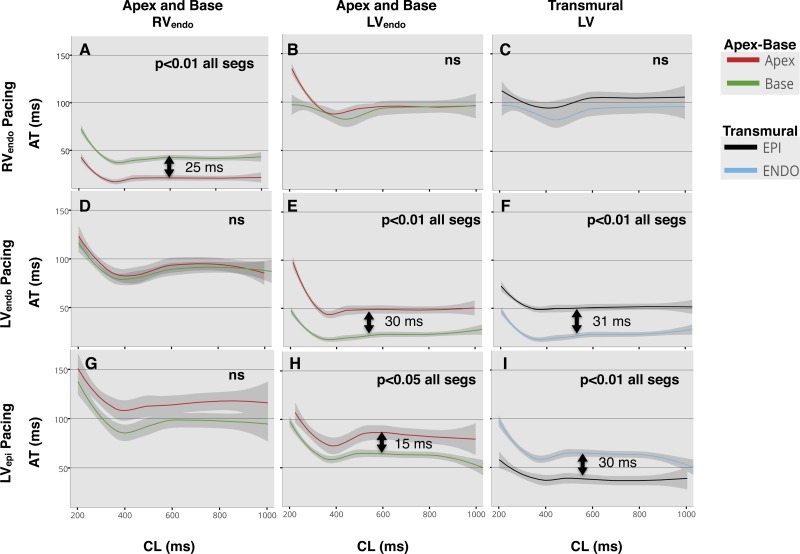
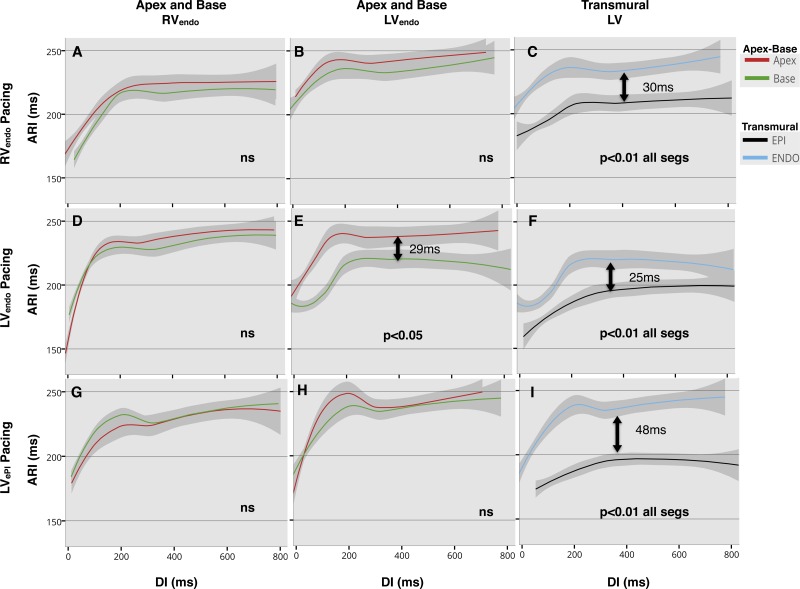
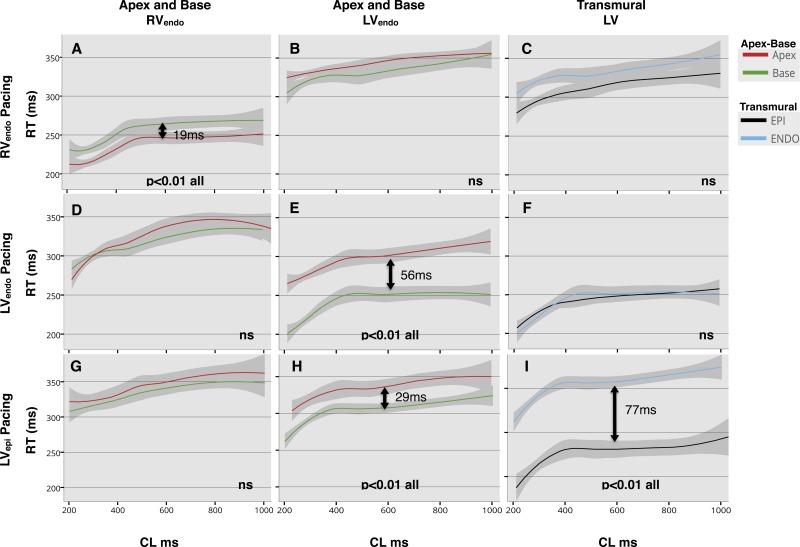
The spatial variation in restitution properties in relation to varying stimulus site is poorly defined. This study aimed to investigate the effect of varying stimulus site on apicobasal and transmural activation time (AT), action potential duration (APD) and repolarization time (RT) during restitution studies in the intact human heart. Ten patients with structurally normal hearts, undergoing clinical electrophysiology studies, were enrolled. Decapolar catheters were placed apex to base in the endocardial right ventricle (RVendo) and left ventricle (LVendo), and an LV branch of the coronary sinus (LVepi) for transmural recording. S1-S2 restitution protocols were performed pacing RVendo apex, LVendo base, and LVepi base. Overall, 725 restitution curves were analyzed, 74% of slopes had a maximum slope of activation recovery interval (ARI) restitution (Smax) > 1 (P < 0.001); mean Smax = 1.76. APD was shorter in the LVepi compared with LVendo, regardless of pacing site (30-ms difference during RVendo pacing, 25-ms during LVendo, and 48-ms during LVepi; 50th quantile, P < 0.01). Basal LVepi pacing resulted in a significant transmural gradient of RT (77 ms, 50th quantile: P < 0.01), due to loss of negative transmural AT-APD coupling (mean slope 0.63 ± 0.3). No significant transmural gradient in RT was demonstrated during endocardial RV or LV pacing, with preserved negative transmural AT-APD coupling (mean slope -1.36 ± 1.9 and -0.71 ± 0.4, respectively). Steep ARI restitution slopes predominate in the normal ventricle and dynamic ARI; RT gradients exist that are modulated by the site of activation. Epicardial stimulation to initiate ventricular activation promotes significant transmural gradients of repolarization that could be proarrhythmic.
Keywords: APD heterogeneity; dispersion of repolarization; human; restitution; whole heart.
Copyright © 2016 the American Physiological Society.
Figures
References
-
- Akar FG. Unique topographical distribution of M cells underlies reentrant mechanism of torsade de pointes in the long-QT syndrome. Circulation 105: 1247–1253, 2002. - PubMed
-
- Antzelevitch C. Electrical heterogeneity, cardiac arrhythmias, and the sodium channel. Circ Res 87: 964–965, 2000. - PubMed
-
- Antzelevitch C, Dumaine R. Electrical heterogeneity in the heart: physiological, pharmacological and clinical implications. In: Comprehensive Physiology, edited by Pollock DM. Hoboken, NJ: Wiley, 2011, p. 654–692.
-
- Antzelevitch C, Sicouri S, Litovsky SH, Lukas A, Krishnan SC, Di Diego JM, Gintant GA, Liu DW. Heterogeneity within the ventricular wall. Electrophysiology and pharmacology of epicardial, endocardial, and M cells. Circ Res 69: 1427–1449, 1991. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous