

Hearing and dementia
- PMID: 27372450
- PMCID: PMC5065893
- DOI: 10.1007/s00415-016-8208-y
Hearing and dementia
Abstract
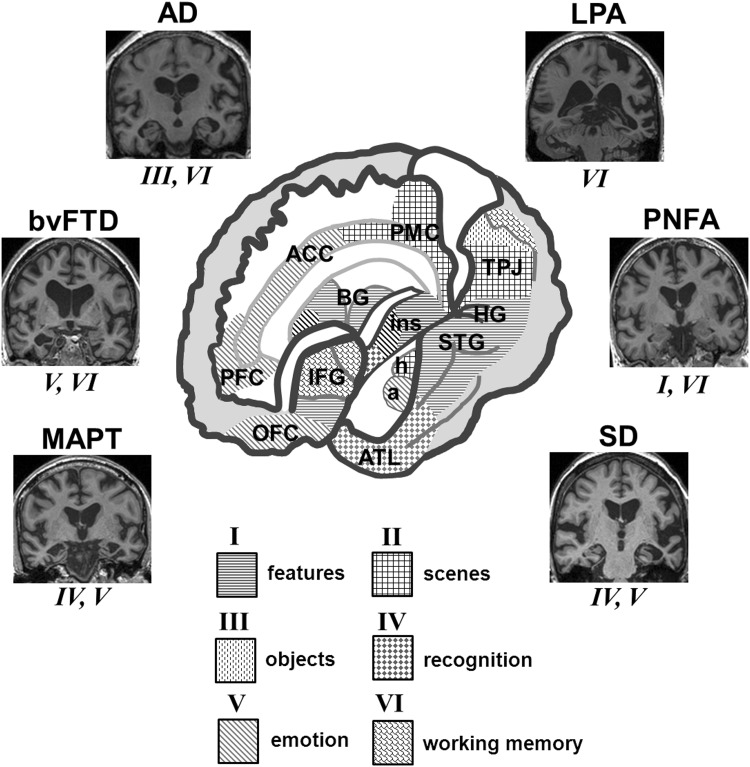
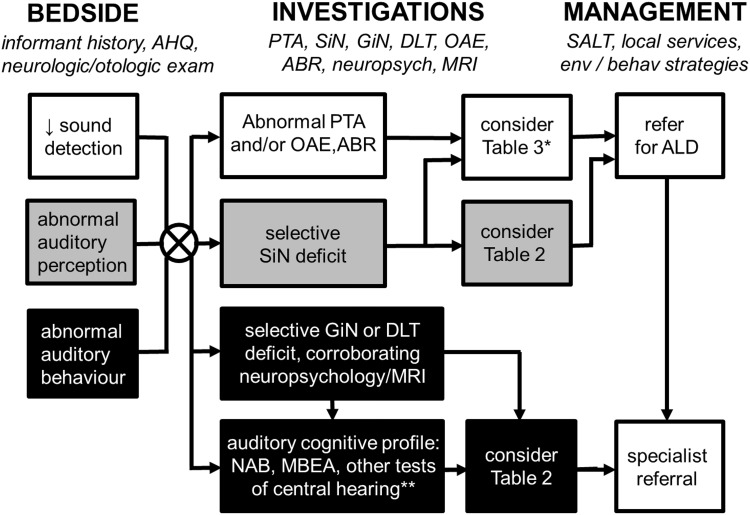
Hearing deficits associated with cognitive impairment have attracted much recent interest, motivated by emerging evidence that impaired hearing is a risk factor for cognitive decline. However, dementia and hearing impairment present immense challenges in their own right, and their intersection in the auditory brain remains poorly understood and difficult to assess. Here, we outline a clinically oriented, symptom-based approach to the assessment of hearing in dementias, informed by recent progress in the clinical auditory neuroscience of these diseases. We consider the significance and interpretation of hearing loss and symptoms that point to a disorder of auditory cognition in patients with dementia. We identify key auditory characteristics of some important dementias and conclude with a bedside approach to assessing and managing auditory dysfunction in dementia.
Keywords: Alzheimer’s disease; Auditory; Dementia; Frontotemporal dementia; Hearing; Lewy body disease; Progressive aphasia.
Conflict of interest statement
Compliance with ethical standards Conflicts of interest The Dementia Research Centre is supported by Alzheimer’s Research UK, the Brain Research Trust and the Wolfson Foundation. CJDH holds an MRC PhD Studentship. CRM is funded by a Clinical Research Fellowship from the Leonard Wolfson Experimental Neurology Centre. HLG was supported by an Alzheimer Research UK PhD Fellowship. CNC is supported by The National Brain Appeal—Frontotemporal Dementia Research Fund. JDW received salary support from the Wellcome Trust (Wellcome Trust Senior Clinical Fellowship (091673/Z/10/Z). The authors report no conflicts of interest. Study funding This work was funded by the Wellcome Trust, the UK Medical Research Council and the NIHR Queen Square Dementia Biomedical Research Unit.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
