

Patients With Hepatocellular Carcinoma Have Highest Rates of Wait-listing for Liver Transplantation Among Patients With End-Stage Liver Disease
- PMID: 27374003
- PMCID: PMC5069141
- DOI: 10.1016/j.cgh.2016.06.019
Patients With Hepatocellular Carcinoma Have Highest Rates of Wait-listing for Liver Transplantation Among Patients With End-Stage Liver Disease
Abstract
Background & aims: Despite recent attention to differences in access to livers for transplantation, research has focused on patients already on the wait list. We analyzed data from a large administrative database that represents the entire US population, and state Medicaid data, to identify factors associated with differences in access to wait lists for liver transplantation.
Methods: We performed a retrospective cohort study of transplant-eligible patients with end-stage liver disease using the HealthCore Integrated Research Database (2006-2014; n = 16,824) and Medicaid data from 5 states (2002-2009; California, Florida, New York, Ohio, and Pennsylvania; n = 67,706). Transplant-eligible patients had decompensated cirrhosis, hepatocellular carcinoma (HCC), and/or liver synthetic dysfunction, based on validated International Classification of Diseases, Ninth Revision-based algorithms and data from laboratory studies. Placement on the wait list was determined through linkage with the Organ Procurement and Transplantation Network database.
Results: In an unadjusted analysis of the HealthCore database, we found that 29% of patients with HCC were placed on the 2-year wait list (95% confidence interval [CI], 25.4%-33.0%) compared with 11.9% of patients with stage 4 cirrhosis (ascites) (95% CI, 11.0%-12.9%) and 12.6% of patients with stage 5 cirrhosis (ascites and variceal bleeding) (95% CI, 9.4%-15.2%). Among patients with each stage of cirrhosis, those with HCC were significantly more likely to be placed on the wait list; adjusted subhazard ratios ranged from 1.7 (for patients with stage 5 cirrhosis and HCC vs those without HCC) to 5.8 (for patients with stage 1 cirrhosis with HCC vs those without HCC). Medicaid beneficiaries with HCC were also more likely to be placed on the transplant wait list, compared with patients with decompensated cirrhosis, with a subhazard ratio of 2.34 (95% CI, 2.20-2.49). Local organ supply and wait list level demand were not associated with placement on the wait list.
Conclusions: In an analysis of US healthcare databases, we found patients with HCC to be more likely to be placed on liver transplant wait lists than patients with decompensated cirrhosis. Previously reported reductions in access to transplant care for wait-listed patients with decompensated cirrhosis underestimate the magnitude of this difference.
Keywords: Disparities; Liver Cancer; UNOS; Wait List.
Copyright © 2016 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
None of the authors have any relevant financial, professional, and/or personal conflicts of interest with respect to this manuscript.
Figures
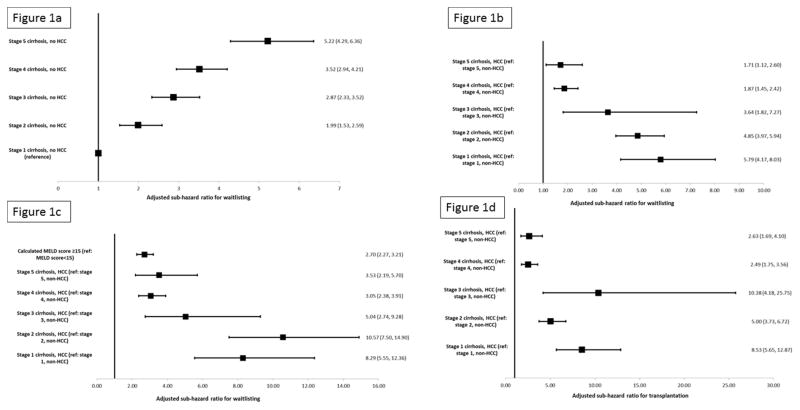
Figure 1a: Adjusted sub-hazard ratios for waitlisting for in HealthCore patients based on time-varying cirrhosis stage in non-HCC patients
Figure 1b: Adjusted sub-hazard ratios for waitlisting for HealthCore patients adjusted for time-varying cirrhosis stage and hepatocellular carcinoma
Figure 1c: Adjusted sub-hazard ratios for waitlisting for HealthCore patients adjusted for time-varying cirrhosis stage, hepatocellular carcinoma, and calculated MELD score*
- i
*Footnote: Sample restricted to all patients with hepatocellular carcinoma and patients with decompensated cirrhosis and laboratory data to calculate the MELD score
- i
Figure 1d: Adjusted sub-hazard ratios for liver transplantation for HealthCore patients adjusted for time-varying cirrhosis stage and hepatocellular carcinoma
References
-
- Goldberg DS, French B, Sahota G, Wallace AE, Lewis JD, Halpern SD. Use of Population-Based Data to Demonstrate How Waitlist-Based Metrics Overestimate Geographic Disparities in Access to Liver Transplant Care. American journal of transplantation: official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2016 - PMC - PubMed
-
- Centers for Medicare and Medicaid Services. [Accessed Accessed April 4, 2012];Medicaid Statistical Information System (MSIS) Tables. 2012 at http://www.cms.gov/MedicaidDataSourcesGenInfo/MSIS/list.asp.
-
- Platt R, Wilson M, Chan KA, Benner JS, Marchibroda J, McClellan M. The new Sentinel Network--improving the evidence of medical-product safety. N Engl J Med. 2009;361:645–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
