

Vascular assessment of wound healing: a clinical review
- PMID: 27374428
- PMCID: PMC7950183
- DOI: 10.1111/iwj.12622
Vascular assessment of wound healing: a clinical review
Abstract
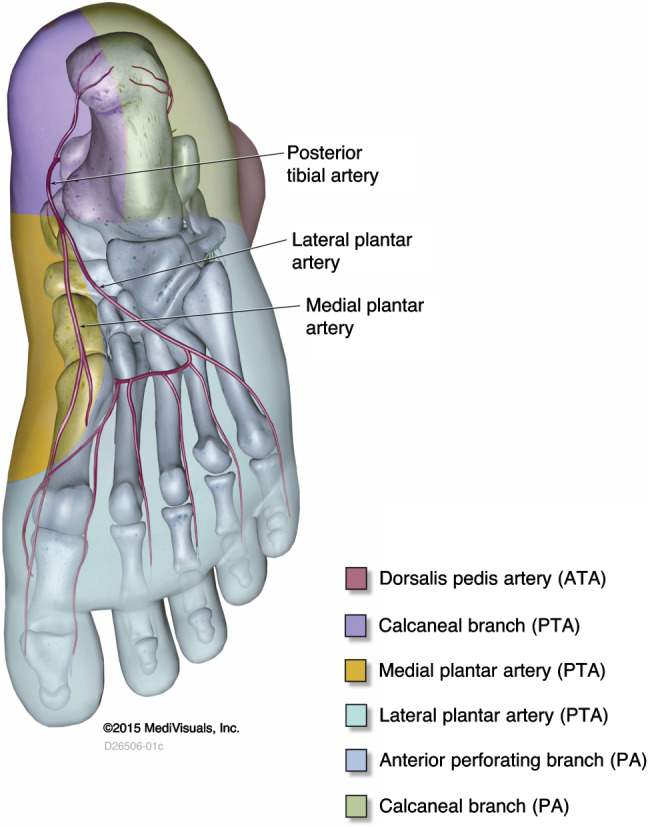
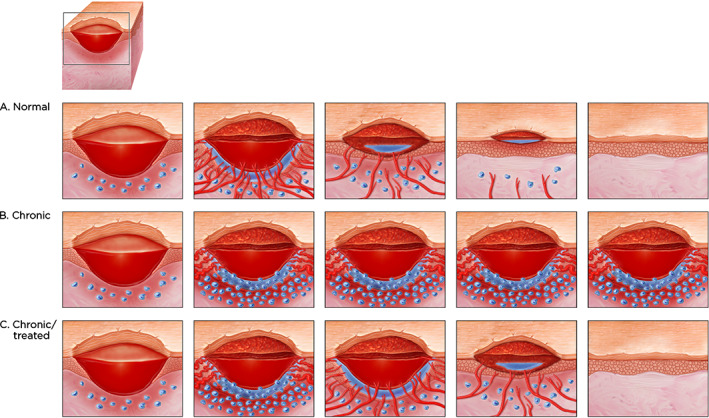
Although macrovascular screening of patients with chronic wounds, particularly in the lower extremities, is accepted as part of clinical practice guidelines, microvascular investigation is less commonly used for a variety of reasons. This can be an issue because most patients with macrovascular disease also develop concomitant microvascular dysfunction. Part of the reason for less comprehensive microvascular screening has been the lack of suitable imaging techniques that can quantify microvascular dysfunction in connection with non-healing chronic wounds. This is changing with the introduction of fluorescence microangiography. The objective of this review is to examine macro- and microvascular disease, the strengths and limitations of the approaches used and to highlight the importance of microvascular angiography in the context of wound healing.
Keywords: Chronic wounds; Fluorescence microangiography; Macrovascular disease; Microvascular dysfunction.
© 2016 Medicalhelplines.com Inc and John Wiley & Sons Ltd.
Figures




References
-
- Lazarus GS, Cooper DM, Knighton DR, Percoraro RE, Rodeheaver G, Robson MC. Definitions and guidelines for assessment of wounds and evaluation of healing. Wound Repair Regen 1994;2:165–70. - PubMed
-
- Sussman C. Management of wound healing with biophysical agent technologies. In: Sussman C, Bates‐Jensen B, editors. Wound care. A practice manual for health professionals, 3rd edn. Baltimore: Lippincott Williams & Wilkins, 2007:498.
-
- Snyder RJ, Driver V, Fife CE, Lantis J, Peirce B, Serena T, Weir D. Using a diagnostic tool to identify elevated protease activity levels in chronic and stalled wounds: a consensus panel discussion. Ostomy Wound Manage 2011;57:36–46. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
