

Lung ultrasound versus chest radiography for the diagnosis of pneumothorax in critically ill patients: A prospective, single-blind study
- PMID: 27375379
- PMCID: PMC4916808
- DOI: 10.4103/1658-354X.174906
Lung ultrasound versus chest radiography for the diagnosis of pneumothorax in critically ill patients: A prospective, single-blind study
Abstract
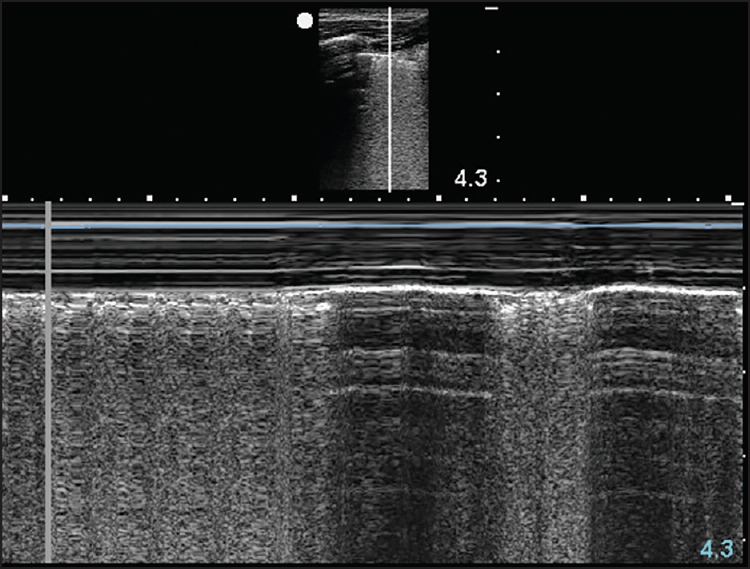
Background: Radiologic data remains the gold standard for the diagnosis of pneumothorax (PTX). The use of ultrasonography (US) has recently emerged as the method of choice with physicians who can perform bedside US.
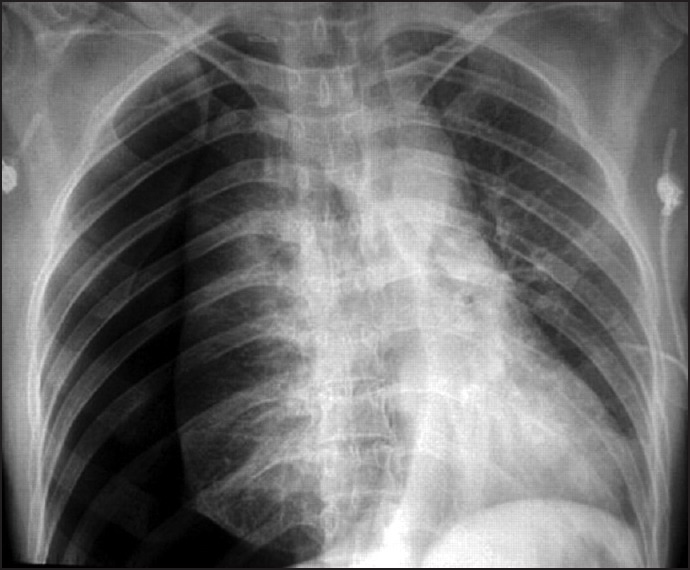
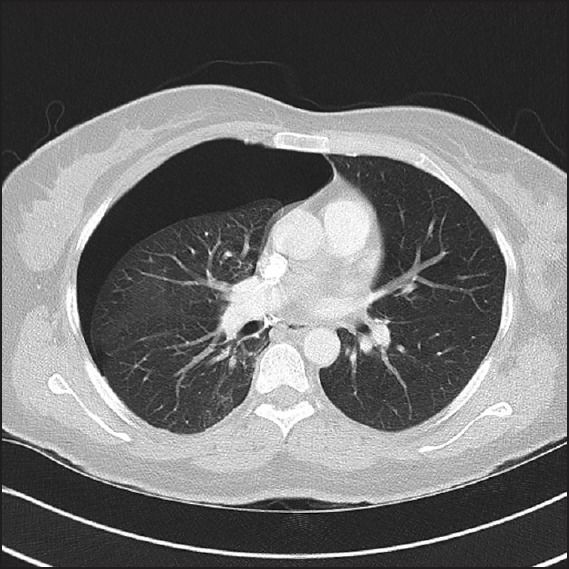
Purpose: To compare the diagnostic accuracy of lung US against bedside chest radiography (CR) for the detection of PTX using thoracic computed tomography (CT) as the gold standard.
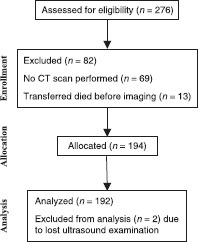
Materials and methods: We conducted a prospective, single-blind study on 192 critically ill patients; each patient received lung US examination, bedside CR, followed by thoracic CT scan searching for PTX.
Results: Of the studied patients, CT of the chest confirmed the diagnosis of PTX in 36 (18.75%) patients of which 31 were diagnosed by thoracic US while CR detected only 19 cases. Overall lung US showed a considerable higher sensitivity than bedside CR (86.1% vs. 52.7%), lung US also showed higher, negative predictive values, and diagnostic accuracy against CR (96.8% vs. 90.1%), and (95.3% vs. 90.6%), respectively. CR had a slightly higher specificity than lung US (99.4% vs. 97.4%), and higher positive predictive values (95.0% vs. 88.6%).
Conclusion: Lung US is an accurate modality more than anteroposterior bedside CR in comparison with CT scanning when evaluating critically ill mechanically ventilated patients, patients underwent thoracocentesis, central venous catheter insertion, or patients with polytrauma.
Keywords: Intensive Care Unit; lung ultrasound; mechanical ventilation; pneumothorax.
Figures

References
-
- Strange C. Pleural complications in the Intensive Care Unit. Clin Chest Med. 1999;20:317–27. - PubMed
-
- de Latorre FJ, Tomasa A, Klamburg J, Leon C, Soler M, Rius J. Incidence of pneumothorax and pneumomediastinum in patients with aspiration pneumonia requiring ventilatory support. Chest. 1977;72:141–4. - PubMed
-
- Wilson H, Ellsmere J, Tallon J, Kirkpatrick A. Occult pneumothorax in the blunt trauma patient: Tube thoracostomy or observation? Injury. 2009;40:928–31. - PubMed
-
- Chiles C, Ravin CE. Radiographic recognition of pneumothorax in the Intensive Care Unit. Crit Care Med. 1986;14:677–80. - PubMed
-
- Tocino IM, Miller MH, Fairfax WR. Distribution of pneumothorax in the supine and semirecumbent critically ill adult. AJR Am J Roentgenol. 1985;144:901–5. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
