

Perceptions of pediatric nephrologists regarding timing of dialysis initiation in children in Canada
- PMID: 27375851
- PMCID: PMC4929756
- DOI: 10.1186/s40697-016-0123-8
Perceptions of pediatric nephrologists regarding timing of dialysis initiation in children in Canada
Abstract
Background: Significant practice variation exists in Canada with respect to timing of dialysis initiation in children. In the absence of evidence to guide practice, physicians' perceptions may significantly influence decision-making.
Objective: The objectives of this study are to (1) evaluate Canadian pediatric nephrologists' perceptions regarding dialysis initiation in children with chronic kidney disease (CKD) and (2) determine the factors guiding practice that may contribute to practice variation across Canada.
Design: This study was a cross-sectional online survey.
Setting: This study was done in academic pediatric nephrology centers in Canada.
Participants: The participants of this study are pediatric nephrologists.
Measurements and methods: An anonymous web-based survey was administered to pediatric nephrologists in Canada to evaluate perspectives and practice patterns regarding timing of dialysis initiation. We also explored the importance of estimated glomerular filtration rate (eGFR) vs. symptoms and the role of patient and provider factors influencing decisions.
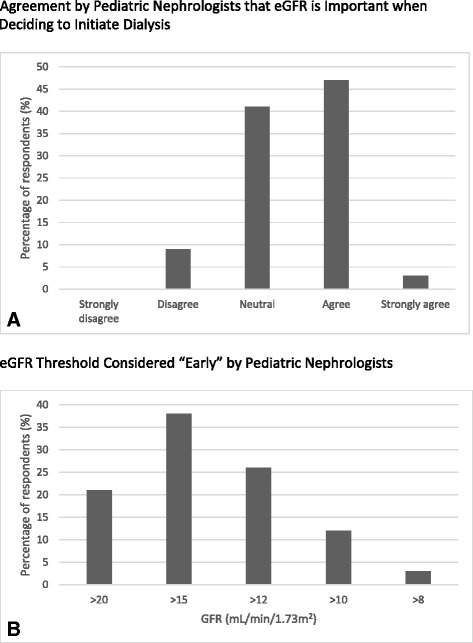
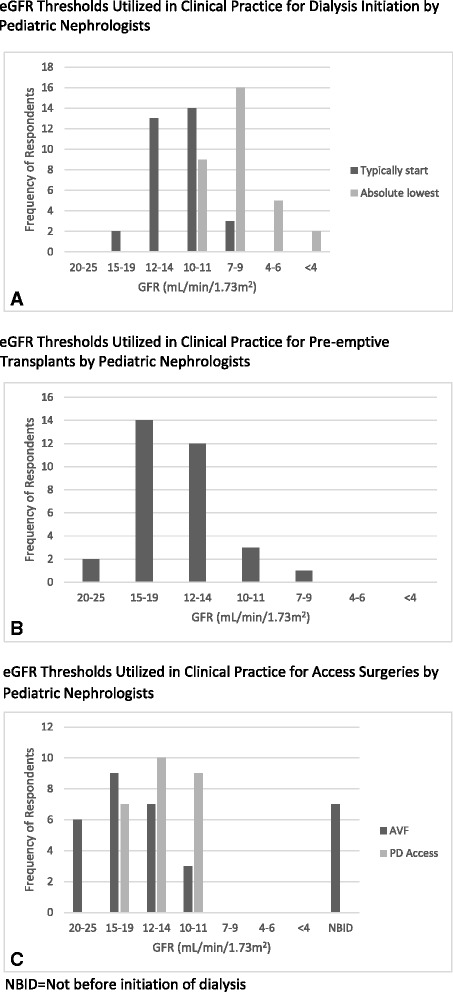
Results: Thirty-five nephrologists (59 %) completed the survey. Most respondents care for advanced CKD patients in a multidisciplinary clinic (86 %) and no centers have a formal policy on timing of dialysis initiation. Seventy-five percent of centers follow <20 stage 4-5 CKD patients, and 9 % follow >30 patients. Discussions about dialysis initiation are generally informal (75 %) and the decision to start is made by the nephrologist (37 %) or a team (57 %). Fifty percent agreed GFR was important when deciding when to initiate dialysis, 41 % were neutral, and 9 % disagreed. Variability exists in the threshold that nephrologists considered early (vs. late) dialysis initiation: >20 (21 %), >15 (38 %), >12 (26 %), and >10 ml/min/1.73 m(2) (12 %). Practitioners however typically start dialysis in asymptomatic patients at eGFRs of 7-9 (9 %), 10-11 (41 %), 12-14 (38 %), and 15-19 (6 %) ml/min/1.73 m(2). Patient factors important in the decision to start dialysis for >90 % of nephrologists were fatigue, >10 % weight loss, nausea, increasing missed school, and awaiting a pre-emptive transplant. Age was only a factor for 56 %.
Limitations: This study has a 59 % response rate.
Conclusions: Variability exists in Canada regarding the importance and threshold of eGFR guiding the decision as to when to start dialysis in children, whereas patient symptoms are almost universally important to pediatric nephrologists' decision-making. Additional studies evaluating outcomes of children starting dialysis earlier vs. later are needed to standardize decision-making and care for children with kidney failure.
Mise en contexte: Des différences significatives existent dans la pratique au Canada quant au moment où des traitements de dialyse devraient être entrepris chez les enfants souffrant d’insuffisance rénale. En absence de données probantes pour guider leur pratique, les différentes approches des néphrologues exerçant auprès de cette population jouent probablement un rôle majeur dans leur prise de décision.
Objectifs de l’étude: Dans un premier temps, l’étude visait à évaluer la perception des néphrologues canadiens en regard de l’amorce de traitements de dialyse chez les enfants atteints d’insuffisance rénale chronique (IRC). Ensuite, on a voulu déterminer les facteurs qui guident la pratique et qui font en sorte que des variations subsistent à cet égard dans la pratique en néphrologie pédiatrique à travers le Canada.
Cadre et type d’étude: Il s’agit d’un sondage transversal mené en ligne auprès des néphrologues pratiquant dans les unités pédiatriques des centres hospitaliers universitaires dans tout le Canada.
Méthodologie: Un sondage accessible par le web, auquel les participants répondaient de façon anonyme, a été distribué aux spécialistes canadiens pratiquant en néphrologie pédiatrique. Ce sondage avait pour objectif d’évaluer les perceptions et les schémas de pratique relativement au moment le plus propice pour amorcer la dialyse. Le sondage explorait aussi l’importance du débit de filtration glomérulaire estimé (DFGe) par rapport aux symptômes ressentis par le patient dans la prise de décision. Finalement, nous avons tenté d’identifier les facteurs pouvant influencer le patient et son médecin traitant au moment de décider d’entreprendre des traitements de dialyse.
Résultats: Tous les pédiatres-néphrologues pratiquant au Canada ont reçu le questionnaire. Toutefois, seulement 35 d’entre eux, soit un peu plus de la moitié (59 %), l’ont complété et renvoyé. La grande majorité des répondants (86 %) exerçaient au sein de cliniques multidisciplinaires, auprès de cas sévères d’IRC. Aucun des centres de soins où ces spécialistes pratiquent ne possédait de politique formelle quant au moment d’entreprendre des traitements de dialyse chez les patients suivis en néphrologie pédiatrique. Les trois quarts des centres de soins cités (75 %) suivaient moins de 20 cas d’IRC de stade 4 ou 5, alors que 9 % en suivaient plus de 30. Les répondants ont indiqué dans une proportion de 75 % que la discussion concernant l’amorce de la dialyse se déroulait de façon informelle. De plus, le sondage révèle que la décision d’amorcer la dialyse est prise par le néphrologue soignant seulement (37 % des cas) ou par une équipe (57 % des cas). La moitié des répondants (50 %) s’accordait pour dire que le DFGe était important dans leur prise de décision d’amorcer des traitements de dialyse chez leurs patients, 41 % avaient une opinion neutre à ce sujet alors que 9 % ne jugeaient pas cet élément important. Les pédiatres-néphrologues répondants sont partagés quant à la valeur seuil de DFGe qu’ils considèrent comme une amorce « hâtive » de dialyse. Pour 21 % des répondants, cette valeur se situe à 20 ml/min/1,73 m2; pour 38 % elle se situe plutôt à 15 ml/min/1,73 m2; 26 % l’établissent à 12 ml/min/1,73 m2; alors que 12 % des répondants jugent l’amorce d’une dialyse dite « hâtive » à un DFGe de 10 ml/min/1,73 m2. De façon générale, chez les patients asymptomatiques, la dialyse est amorcée lorsque le DFGe se situe entre 7 et 9 ml/min/1,73 m2 (9 % des cas), entre 10 et 11 ml/min/1,73 m2 (41 % des cas), entre 12 et 14 ml/min/1,73 m2 (38 % des cas) ou entre 15 et 19 ml/min/1,73 m2 (6 % des cas). Enfin, parmi les facteurs motivant les patients à entreprendre des traitements de dialyse, tels que rapportés par les répondants dans une proportion de plus de 90 %, on trouve : une sensation de fatigue, une perte de poids de plus de 10 %, des nausées, les absences répétées à l’école et l’attente d’une greffe rénale préventive. L’âge n’a été mentionné comme facteur que dans 56 % des cas.
Limites de l’étude: Le taux de réponse au sondage relativement faible (59 %) limite la portée des résultats.
Conclusions: En néphrologie pédiatrique, alors que les symptômes ressentis par les patients sont considérés de façon universelle dans la décision d’entreprendre une dialyse, les pédiatres-néphrologues canadiens ont des perceptions très différentes quant à la valeur seuil de DFGe qui devrait guider cette décision et à l’importance du rôle que ce paramètre devrait y jouer. Des études supplémentaires comparant les résultats chez les patients qui amorcent une dialyse dite hâtive par rapport à ceux de patients l’amorçant plus tard s’avèrent nécessaires pour établir des pratiques standardisées en matière de soins pour les enfants atteints d’insuffisance rénale.
Figures
References
-
- CIHI . Canadian organ replacement register annual report: treatment of end-stage organ failure in Canada, 2002 to 2011. Ottawa, ON: CIHI; 2012.
-
- Dart AB SS, Sood MM, Alexander RT, Arora S, Erickson RL, Manns BJ, Zappitelli M. Variability in timing of dialysis initiation in children. Atlanta, Georgia: American Society of Nephrology Renal Week; 2013.
-
- Hakim RM, Lazarus JM. Initiation of dialysis. J Am Soc Nephrol. 1995;6(5):1319–28. - PubMed
-
- Bonomini V, Vangelista A, Stefoni S. Early dialysis in renal substitutive programs. Kidney Int Suppl. 1978;8:S112–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
