

Benefit of Adjuvant Chemotherapy and Pelvic Lymph Node Dissection in pT3 and Node Positive Bladder Cancer Patients Treated with Radical Cystectomy
- PMID: 27376145
- PMCID: PMC4927915
- DOI: 10.3233/BLC-150032
Benefit of Adjuvant Chemotherapy and Pelvic Lymph Node Dissection in pT3 and Node Positive Bladder Cancer Patients Treated with Radical Cystectomy
Abstract
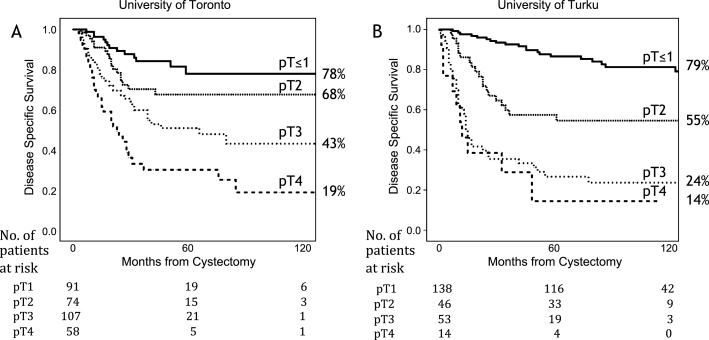
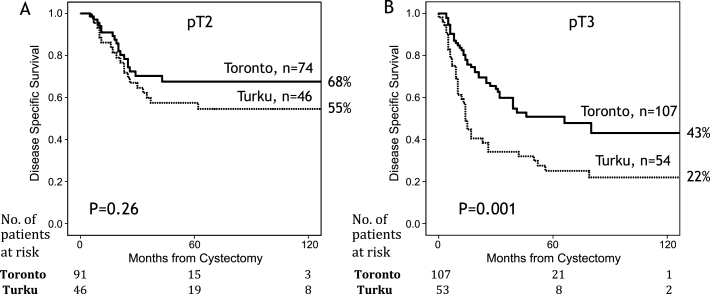
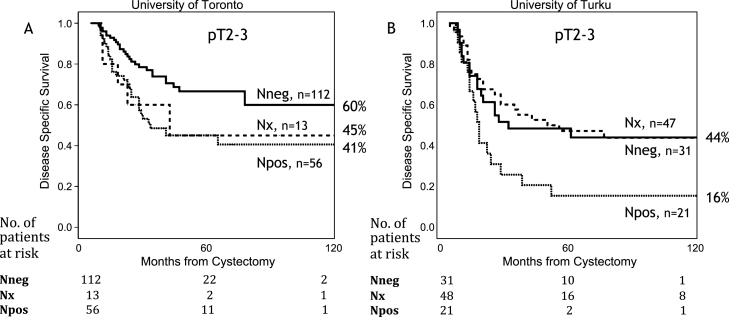
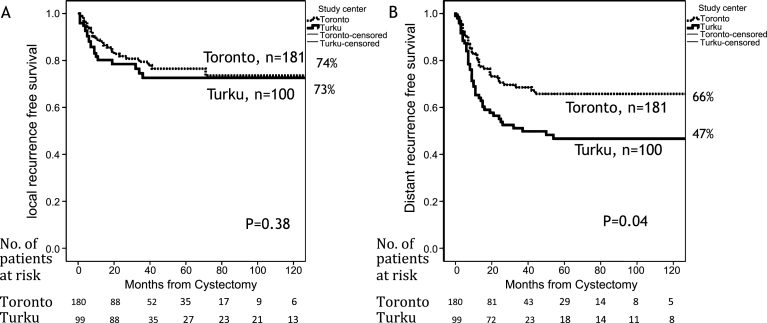
Background: Benefits of adjuvant chemotherapy (AC) and extent of pelvic lymph node dissection (PLND) in radical cystectomy (RC) are debated. Results from randomized trials are still expected. Objective: To analyze the effects of AC and PLND in two academic centers with opposite policies regarding their use. Methods: 581 bladder cancer patients who underwent RC without neoadjuvant chemotherapy, from Toronto (University Health Network), Canada, and Turku University Hospital, Finland were included. Disease specific survival (DSS) and failure patterns were assessed. Results: Centers differed in PLND rate (93% and 36% in Toronto and Turku respectively, p < 0.001), PLND extent (≥10 removed nodes, 58% vs. 8%, p < 0.001) and AC rate (21% vs. 2%, p < 0.001). Survival between centers among pT≤1 or pT4 patients was similar. pT3 patients in Toronto had an improved 10 year DSS (43% vs. 22%, p = 0.025). Distant failures were less common after AC (HR 0.56, 95% CI 0.33-0.98, p < 0.042). In node positive (N+) patients, mortality was significantly higher in Turku (HR 2.19, 95% CI 1.44-3.34, p < 0.001) and lower in patients receiving AC (HR 0.60, 95% CI 0.37-0.99, p = 0.044). 41% DSS at 10 years was observed in N+ Toronto patients. Limitations included the non-randomized retrospective design and absence of propensity score analysis. Conclusion: Combining AC and PLND to RC is associated with improved survival in pT3 and N+ patients. PLND did not affect survival independently but helps in selecting patients for AC. Our data adds to the growing body of evidence supporting the usefulness of AC in addition to PLND in high risk patients operated by cystectomy.
Keywords: Bladder cancer; adjuvant chemotherapy; lymphadenectomy; radical cystectomy.
Figures
Similar articles
-
Extended versus standard lymph node dissection for urothelial carcinoma of the bladder in patients undergoing radical cystectomy.Cochrane Database Syst Rev. 2019 May 14;5(5):CD013336. doi: 10.1002/14651858.CD013336. Cochrane Database Syst Rev. 2019. PMID: 31111956 Free PMC article.
-
Effectiveness of Adjuvant Chemotherapy After Radical Cystectomy for Locally Advanced and/or Pelvic Lymph Node-Positive Muscle-invasive Urothelial Carcinoma of the Bladder: A Propensity Score-Weighted Competing Risks Analysis.Eur Urol Focus. 2018 Mar;4(2):252-259. doi: 10.1016/j.euf.2016.07.001. Epub 2016 Jul 18. Eur Urol Focus. 2018. PMID: 28753775
-
Prediction of the Need for an Extended Lymphadenectomy at the Time of Radical Cystectomy in Patients with Bladder Cancer.Eur Urol Focus. 2021 Sep;7(5):1067-1074. doi: 10.1016/j.euf.2020.09.009. Epub 2020 Oct 2. Eur Urol Focus. 2021. PMID: 33020030 Clinical Trial.
-
Differential effect on survival of pelvic lymph node dissection at radical cystectomy for muscle invasive bladder cancer.Eur J Surg Oncol. 2015 Mar;41(3):353-60. doi: 10.1016/j.ejso.2014.10.061. Epub 2014 Nov 21. Eur J Surg Oncol. 2015. PMID: 25477269
-
Adequate Pelvic Lymph Node Dissection in Radical Cystectomy in the Era of Neoadjuvant Chemotherapy: A Meta-Analysis and Systematic Review.Cancers (Basel). 2023 Aug 10;15(16):4040. doi: 10.3390/cancers15164040. Cancers (Basel). 2023. PMID: 37627068 Free PMC article. Review.
Cited by
-
Management of Bladder Cancer Patients with Clinical Evidence of Lymph Node Invasion (cN+).Cancers (Basel). 2022 Oct 27;14(21):5286. doi: 10.3390/cancers14215286. Cancers (Basel). 2022. PMID: 36358705 Free PMC article. Review.
-
Dissecting the role of lymphadenectomy in the management of renal cell carcinoma: past, present, and future.Kidney Cancer J. 2020 Dec;18(4):103-108. Kidney Cancer J. 2020. PMID: 35069965 Free PMC article.
-
Peri-operative chemotherapy for muscle-invasive bladder cancer: status-quo in 2017.Transl Androl Urol. 2017 Dec;6(6):1049-1059. doi: 10.21037/tau.2017.09.12. Transl Androl Urol. 2017. PMID: 29354492 Free PMC article. Review.
-
Clinicopathological factors in bladder cancer for cancer-specific survival outcomes following radical cystectomy: a systematic review and meta-analysis.BMC Cancer. 2019 Jul 19;19(1):716. doi: 10.1186/s12885-019-5924-6. BMC Cancer. 2019. PMID: 31324162 Free PMC article.
References
-
- Stein J, Lieskovsky G, Cote R, Groshen S, Feng AC, Boyd S, Skinner E, Bochner B, Thangathurai D, Mikhail M, Raghavan D, Skinner DG. Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1,054 patients. J Clin Oncol 2001;19:666–75. - PubMed
-
- Madersbacher S, Hochreiter W, Burkhard F, Thalmann GN, Danuser H, Markwalder R, Studer UE. Radical cystectomy for bladder cancer today–a homogeneous series without neoadjuvant therapy. J Clin Oncol 2003;21:690–6. - PubMed
-
- Hautmann R, Gschwend J, de Petriconi R, Kron M, Volkmer BG. Cystectomy for transitional cell carcinoma of the bladder: Results of a surgery only series in the neobladder era. J Urol 2006;176:486–92. - PubMed
-
- Shariat S, Karakiewicz P, Palapattu G, Lotan Y, Rogers CG, Amiel GE, Vazina A, Gupta A, Bastian PJ, Sagalowsky AI, Schoenberg MP, Lerner SP. Outcomes of radical cystectomy for transitional cell carcinoma of the bladder: A contemporary series from the Bladder Cancer Research Consortium. J Urol 2006;176:2414–22. - PubMed
-
- Sternberg CN, Skoneczna I, Kerst JM, Albers P, Fossa SD, Agerbaek M, Dumez H, de Santis M, Théodore C, Leahy MG, Chester JD, Verbaeys A, Daugaard G, Wood L, Witjes JA, de Wit R, Geoffrois L, Sengelov L, Thalmann G, Charpentier D, Rolland F, Mignot L, Sundar S, Symonds P, Graham J, Joly F, Marreaud S, Collette L, Sylvester R. Immediate versus deferred chemotherapy after radical cystectomy in patients with pT3-pT4 or N+ M0 urothelial carcinoma of the bladder (EORTC 30994): An intergroup, open-label, randomised phase 3 trial. Lancet Oncol 2015;16(1), 76–86. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
