

Development of the Canadian Syncope Risk Score to predict serious adverse events after emergency department assessment of syncope
- PMID: 27378464
- PMCID: PMC5008955
- DOI: 10.1503/cmaj.151469
Development of the Canadian Syncope Risk Score to predict serious adverse events after emergency department assessment of syncope
Abstract
Background: Syncope can be caused by serious conditions not evident during initial evaluation, which can lead to serious adverse events, including death, after disposition from the emergency department. We sought to develop a clinical decision tool to identify adult patients with syncope who are at risk of a serious adverse event within 30 days after disposition from the emergency department.
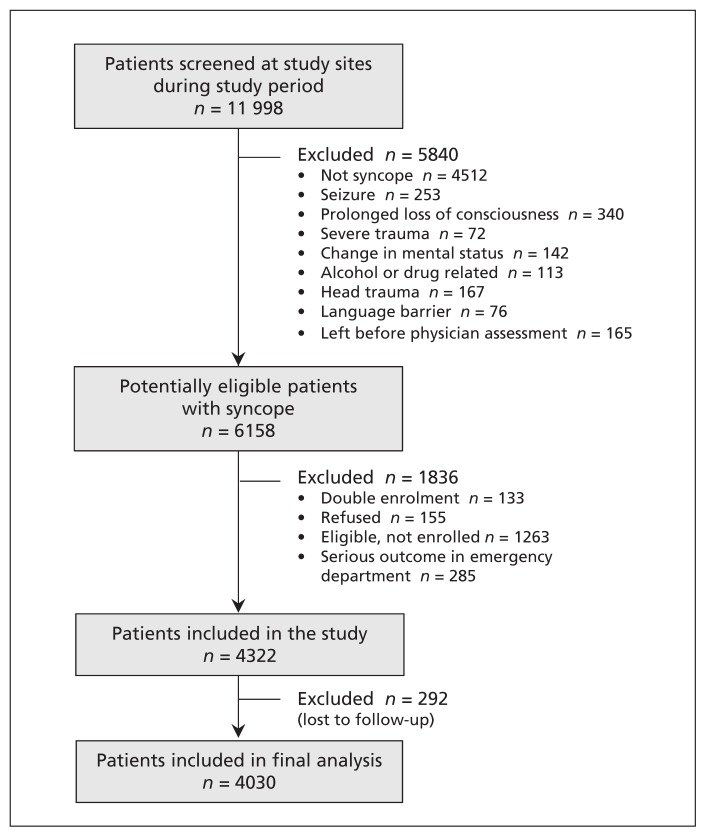
Methods: We prospectively enrolled adults (age ≥ 16 yr) with syncope who presented within 24 hours after the event to 1 of 6 large emergency departments from Sept. 29, 2010, to Feb. 27, 2014. We collected standardized variables at index presentation from clinical evaluation and investigations. Adjudicated serious adverse events included death, myocardial infarction, arrhythmia, structural heart disease, pulmonary embolism, serious hemorrhage and procedural interventions within 30 days.
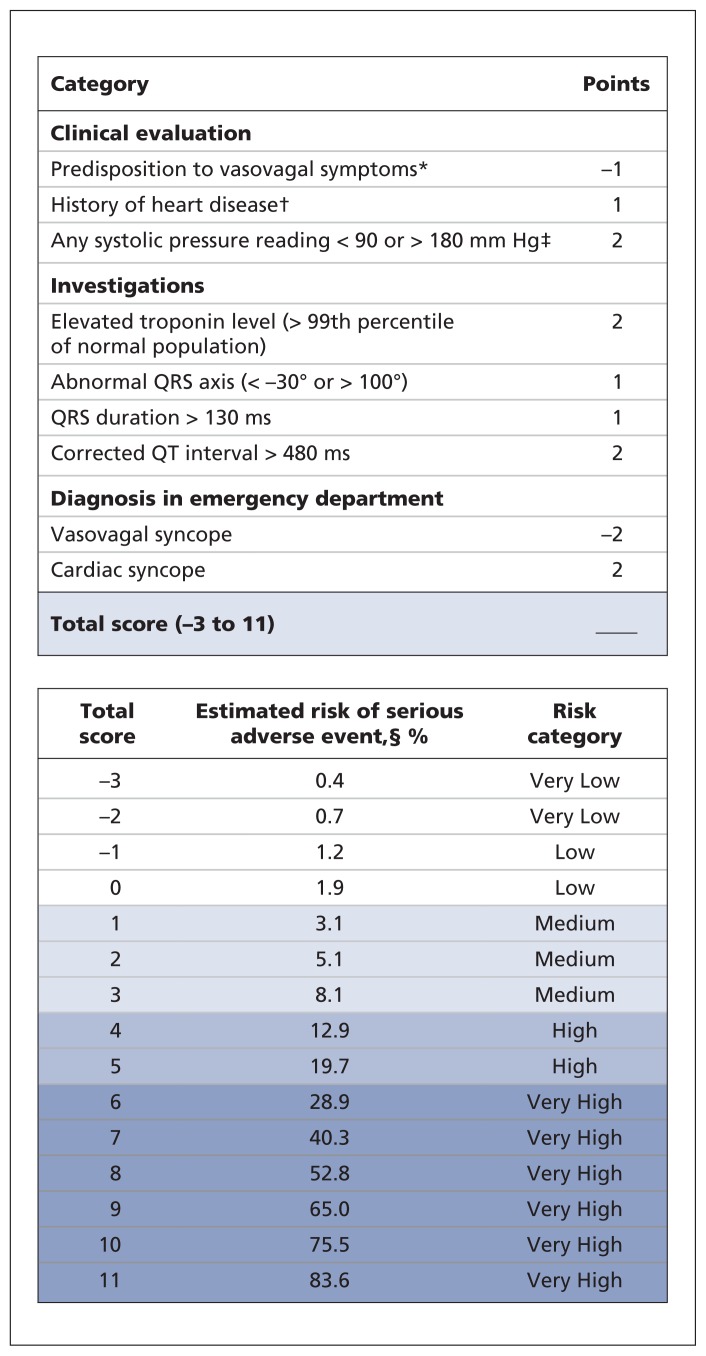
Results: We enrolled 4030 patients with syncope; the mean age was 53.6 years, 55.5% were women, and 9.5% were admitted to hospital. Serious adverse events occurred in 147 (3.6%) of the patients within 30 days after disposition from the emergency department. Of 43 candidate predictors examined, we included 9 in the final model: predisposition to vasovagal syncope, heart disease, any systolic pressure reading in the emergency department < 90 or > 180 mm Hg, troponin level above 99th percentile for the normal population, abnormal QRS axis (< -30° or > 100°), QRS duration longer than 130 ms, QTc interval longer than 480 ms, emergency department diagnosis of cardiac syncope and emergency department diagnosis of vasovagal syncope (C statistic 0.88, 95% confidence interval [CI] 0.85-0.90; optimism 0.015; goodness-of-fit p = 0.11). The risk of a serious adverse event within 30 days ranged from 0.4% for a score of -3 to 83.6% for a score of 11. The sensitivity was 99.2% (95% CI 95.9%-100%) for a threshold score of -2 or higher and 97.7% (95% CI 93.5%-99.5%) for a threshold score of -1 or higher.
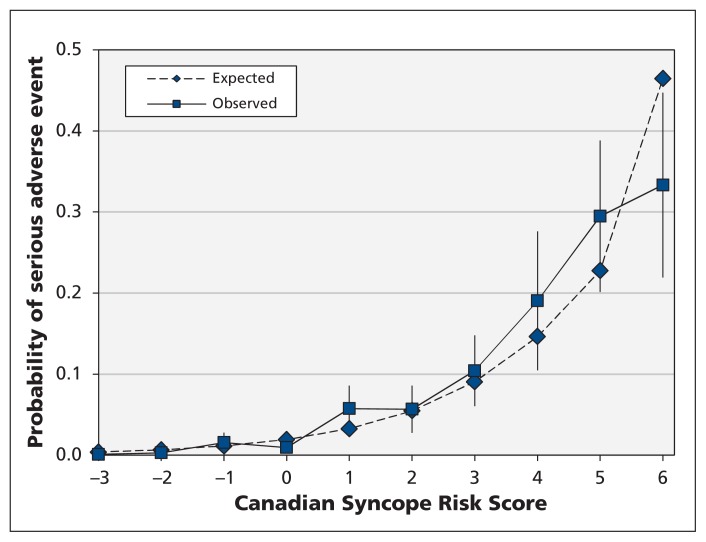
Interpretation: The Canadian Syncope Risk Score showed good discrimination and calibration for 30-day risk of serious adverse events after disposition from the emergency department. Once validated, the tool will be able to accurately stratify the risk of serious adverse events among patients presenting with syncope, including those at low risk who can be discharged home quickly.
© 2016 Canadian Medical Association or its licensors.
Figures
References
-
- Blanc JJ, L’Her C, Touiza A, et al. Prospective evaluation and outcome of patients admitted for syncope over a 1 year period. Eur Heart J 2002;23:815–20. - PubMed
-
- Sun BC, Emond JA, Camargo CA., Jr Characteristics and admission patterns of patients presenting with syncope to US emergency departments, 1992–2000. Acad Emerg Med 2004;11:1029–34. - PubMed
-
- Ganzeboom KS, Mairuhu G, Reitsma JB, et al. Lifetime cumulative incidence of syncope in the general population: a study of 549 Dutch subjects aged 35–60 years. J Cardiovasc Electrophysiol 2006;17:1172–6. - PubMed
-
- Kapoor WN. Evaluation and outcome of patients with syncope. Medicine 1990;69:160–75. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical