

A Prospective Surveillance Study of Candidaemia: Epidemiology, Risk Factors, Antifungal Treatment and Outcome in Hospitalized Patients
- PMID: 27379047
- PMCID: PMC4910670
- DOI: 10.3389/fmicb.2016.00915
A Prospective Surveillance Study of Candidaemia: Epidemiology, Risk Factors, Antifungal Treatment and Outcome in Hospitalized Patients
Abstract
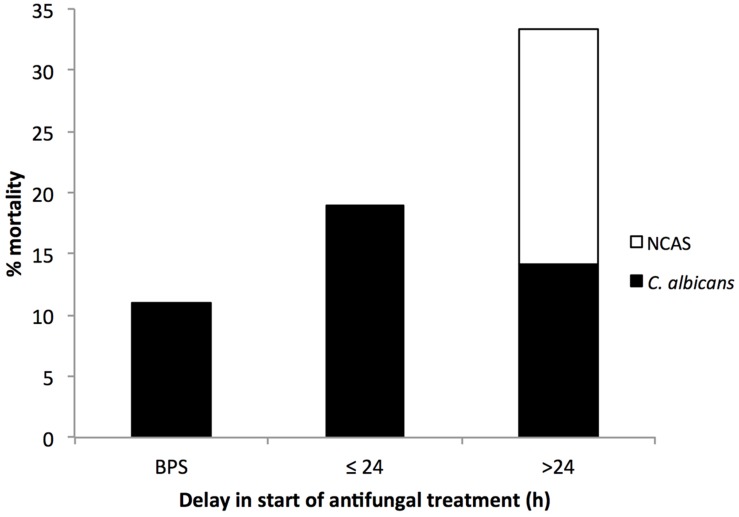
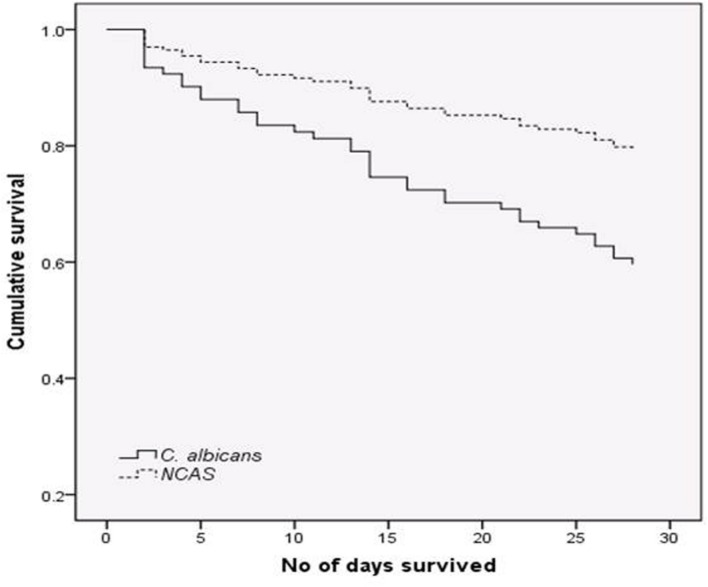
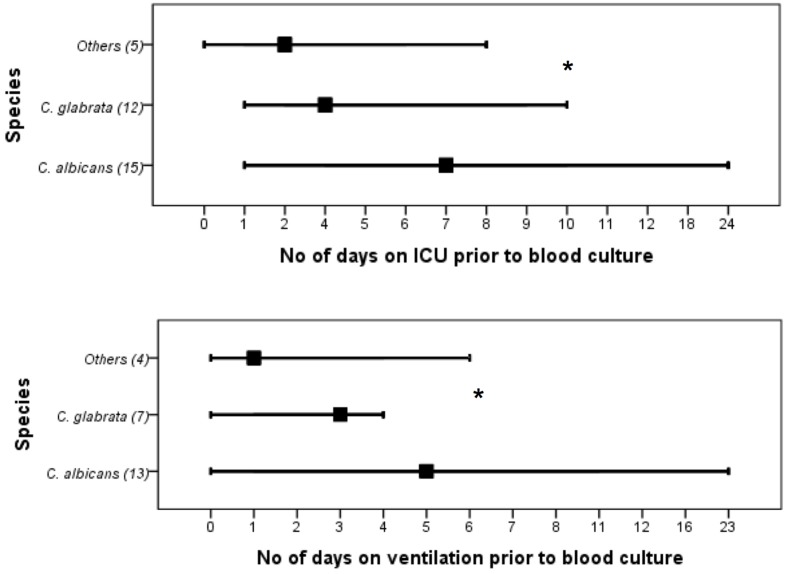
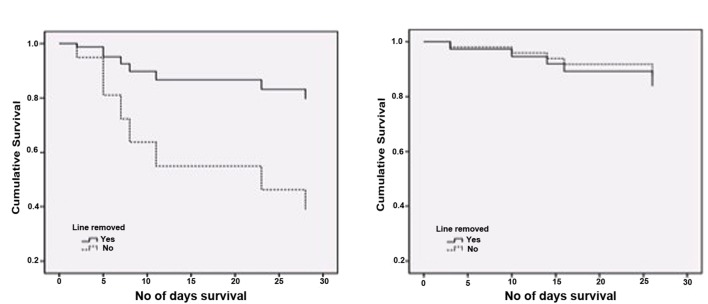
This study provide an up-to-date overview of the epidemiology and risk factors for Candida bloodstream infection in Scotland in 2012/2013, and the antifungal susceptibility of isolates from blood cultures from 11 National Health Service boards within Scotland. Candida isolates were identified by chromogenic agar and confirmed by MALDI-TOF methods. Survival and associated risk factors for patients stratified as albicans and non-albicans cases were assessed. Information on the spectrum of antifungals used was collected and summarized. The isolates sensitivity to different antifungals was tested by broth microdilution method and interpreted according to CLSI/EUCAST guidelines. Forty one percent of candidaemia cases were associated with Candida albicans, followed by C. glabrata (35%), C. parapsilosis (11.5%), and remainder with other Candida spp. C. albicans and C. glabrata infections were associated with 20.9 and 16.3% mortality, respectively. Survival of patients with C. albicans was significantly lower compared to non-C. albicans and catheter line removal in C. albicans patients significantly increases the survival days. Predisposing factors such as total parenteral nutrition, and number of days on mechanical ventilation or in intensive care, were significantly associated with C. albicans infections. Fluconazole was used extensively (64.5%) for treating candidaemia cases followed by echinocandins (33.8%). Based on CLSI breakpoints, MIC test found no resistance to any antifungals tested except 5.26% fluconazole resistance among C. glabrata isolates. Moreover, by comparing to EUCAST breakpoints we found 3.95% of C. glabrata isolates were resistant to anidulafungin. We have observed a shift in Candida spp. with an increasing isolation of C. glabrata. Delay and choice of antifungal treatment are associated with poor clinical outcomes.
Keywords: Candida albicans; Candida glabrata; antifungals; candidaemia; drug resistance.
Figures
References
-
- Almirante B., Rodriguez D., Park B. J., Cuenca-Estrella M., Planes A. M., Almela M., et al. (2005). Epidemiology and predictors of mortality in cases of Candida bloodstream infection: results from population-based surveillance, barcelona, Spain, from 2002 to 2003. J. Clin. Microbiol. 43 1829–1835. 10.1128/JCM.43.4.1829-1835.2005 - DOI - PMC - PubMed
-
- Arendrup M. C., Dzajic E., Jensen R. H., Johansen H. K., Kjaeldgaard P., Knudsen J. D., et al. (2013b). Epidemiological changes with potential implication for antifungal prescription recommendations for fungaemia: data from a nationwide fungaemia surveillance programme. Clin. Microbiol. Infect. 19:E343–E353. 10.1111/1469-0691.12212 - DOI - PubMed
-
- Castanheira M., Messer S. A., Rhomberg P. R., Pfaller M. A. (2016). Antifungal susceptibility patterns of a global collection of fungal isolates: results of the SENTRY antifungal surveillance program (2013). Diagn. Microbiol. Infect. Dis. 85 200–204. 10.1016/j.diagmicrobio.2016.02.009 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous