

Neurological Sequelae Resulting from Encephalitic Alphavirus Infection
- PMID: 27379085
- PMCID: PMC4913092
- DOI: 10.3389/fmicb.2016.00959
Neurological Sequelae Resulting from Encephalitic Alphavirus Infection
Abstract
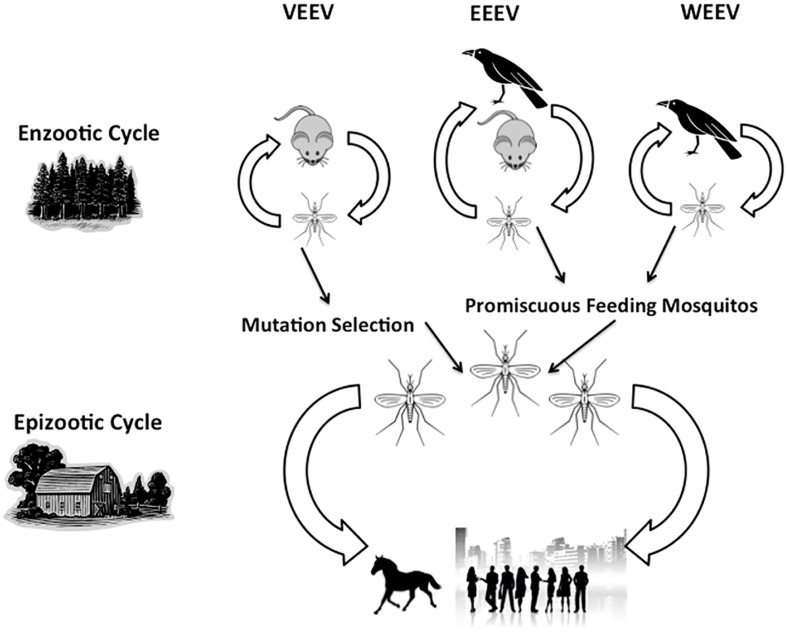
The recent surge in viral clinical cases and associated neurological deficits have reminded us that viral infections can lead to detrimental, long-term effects, termed sequelae, in survivors. Alphaviruses are enveloped, single-stranded positive-sense RNA viruses in the Togaviridae family. Transmission of alphaviruses between and within species occurs mainly via the bite of an infected mosquito bite, giving alphaviruses a place among arboviruses, or arthropod-borne viruses. Alphaviruses are found throughout the world and typically cause arthralgic or encephalitic disease in infected humans. Originally detected in the 1930s, today the major encephalitic viruses include Venezuelan, Western, and Eastern equine encephalitis viruses (VEEV, WEEV, and EEEV, respectively). VEEV, WEEV, and EEEV are endemic to the Americas and are important human pathogens, leading to thousands of human infections each year. Despite awareness of these viruses for nearly 100 years, we possess little mechanistic understanding regarding the complications (sequelae) that emerge after resolution of acute infection. Neurological sequelae are those complications involving damage to the central nervous system that results in cognitive, sensory, or motor deficits that may also manifest as emotional instability and seizures in the most severe cases. This article serves to provide an overview of clinical cases documented in the past century as well as a summary of the reported neurological sequelae due to VEEV, WEEV, and EEEV infection. We conclude with a treatise on the utility of, and practical considerations for animal models applied to the problem of neurological sequelae of viral encephalopathies in order to decipher mechanisms and interventional strategies.
Keywords: VEEV; WEEV; alphavirus; behavior; sequelae.
Figures
References
-
- Alevizatos A. C., McKinney R. W., Feigin R. D. (1967). Live, attenuated Venezuelan equine encephalomyelitis virus vaccine. I. Clinical effects in man. Am. J. Trop. Med. Hyg. 16 762–768. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous