

Association of Specific Dietary Fats With Total and Cause-Specific Mortality
- PMID: 27379574
- PMCID: PMC5123772
- DOI: 10.1001/jamainternmed.2016.2417
Association of Specific Dietary Fats With Total and Cause-Specific Mortality
Abstract
Importance: Previous studies have shown distinct associations between specific dietary fat and cardiovascular disease. However, evidence on specific dietary fat and mortality remains limited and inconsistent.
Objective: To examine the associations of specific dietary fats with total and cause-specific mortality in 2 large ongoing cohort studies.
Design, setting, and participants: This cohort study investigated 83 349 women from the Nurses' Health Study (July 1, 1980, to June 30, 2012) and 42 884 men from the Health Professionals Follow-up Study (February 1, 1986, to January 31, 2012) who were free of cardiovascular disease, cancer, and types 1 and 2 diabetes at baseline. Dietary fat intake was assessed at baseline and updated every 2 to 4 years. Information on mortality was obtained from systematic searches of the vital records of states and the National Death Index, supplemented by reports from family members or postal authorities. Data were analyzed from September 18, 2014, to March 27, 2016.
Main outcomes and measures: Total and cause-specific mortality.
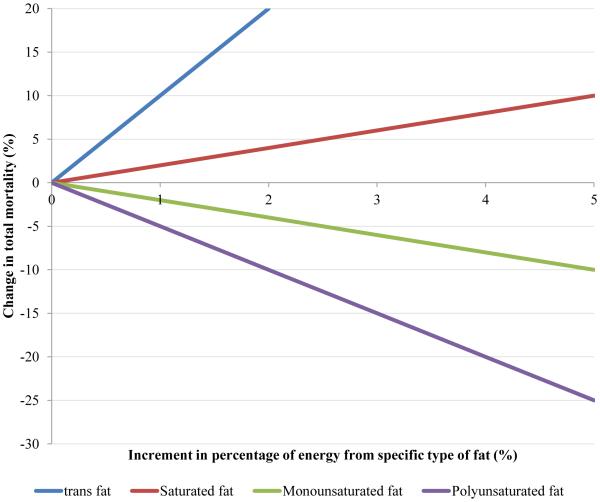
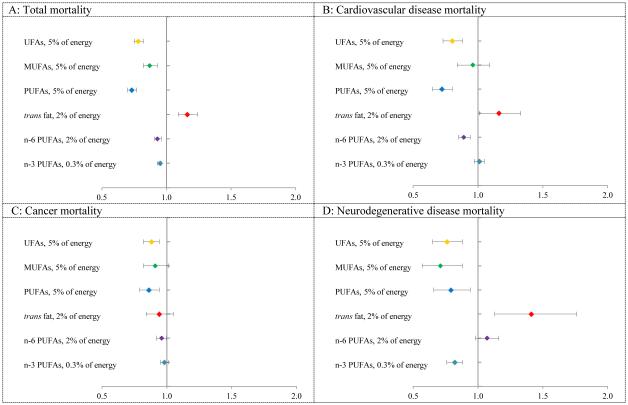
Results: During 3 439 954 person-years of follow-up, 33 304 deaths were documented. After adjustment for known and suspected risk factors, dietary total fat compared with total carbohydrates was inversely associated with total mortality (hazard ratio [HR] comparing extreme quintiles, 0.84; 95% CI, 0.81-0.88; P < .001 for trend). The HRs of total mortality comparing extreme quintiles of specific dietary fats were 1.08 (95% CI, 1.03-1.14) for saturated fat, 0.81 (95% CI, 0.78-0.84) for polyunsaturated fatty acid (PUFA), 0.89 (95% CI, 0.84-0.94) for monounsaturated fatty acid (MUFA), and 1.13 (95% CI, 1.07-1.18) for trans-fat (P < .001 for trend for all). Replacing 5% of energy from saturated fats with equivalent energy from PUFA and MUFA was associated with estimated reductions in total mortality of 27% (HR, 0.73; 95% CI, 0.70-0.77) and 13% (HR, 0.87; 95% CI, 0.82-0.93), respectively. The HR for total mortality comparing extreme quintiles of ω-6 PUFA intake was 0.85 (95% CI, 0.81-0.89; P < .001 for trend). Intake of ω-6 PUFA, especially linoleic acid, was inversely associated with mortality owing to most major causes, whereas marine ω-3 PUFA intake was associated with a modestly lower total mortality (HR comparing extreme quintiles, 0.96; 95% CI, 0.93-1.00; P = .002 for trend).
Conclusions and relevance: Different types of dietary fats have divergent associations with total and cause-specific mortality. These findings support current dietary recommendations to replace saturated fat and trans-fat with unsaturated fats.
Figures
Comment in
-
Association of Specific Dietary Fats With Mortality.JAMA Intern Med. 2016 Dec 1;176(12):1878. doi: 10.1001/jamainternmed.2016.7125. JAMA Intern Med. 2016. PMID: 27918809 No abstract available.
-
Association of Specific Dietary Fats With Mortality.JAMA Intern Med. 2016 Dec 1;176(12):1878-1879. doi: 10.1001/jamainternmed.2016.7131. JAMA Intern Med. 2016. PMID: 27918810 No abstract available.
-
Association of Specific Dietary Fats With Mortality-Reply.JAMA Intern Med. 2016 Dec 1;176(12):1879-1880. doi: 10.1001/jamainternmed.2016.7137. JAMA Intern Med. 2016. PMID: 27918817 No abstract available.
-
Lingering Questions Concerning Specific Dietary Fats and Mortality.JAMA Intern Med. 2017 Apr 1;177(4):596-597. doi: 10.1001/jamainternmed.2017.0040. JAMA Intern Med. 2017. PMID: 28384763 No abstract available.
-
Lingering Questions Concerning Specific Dietary Fats and Mortality-Reply.JAMA Intern Med. 2017 Apr 1;177(4):597-598. doi: 10.1001/jamainternmed.2017.0043. JAMA Intern Med. 2017. PMID: 28384769 No abstract available.
References
-
- Willett WC. Dietary fats and coronary heart disease. J Intern Med. 2012 Jul;272(1):13–24. - PubMed
-
- Hu FB, Stampfer MJ, Manson JE, et al. Dietary fat intake and the risk of coronary heart disease in women. N Engl J Med. 1997 Nov 20;337(21):1491–1499. - PubMed
-
- Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2010 Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2010, to the Secretary of Agriculture and the Secretary of Health and Human Services. Agricultural Research Service. 2010
-
- Chowdhury R, Warnakula S, Kunutsor S, et al. Association of dietary, circulating, and supplement fatty acids with coronary risk: a systematic review and meta-analysis. Ann Intern Med. 2014 Mar 18;160(6):398–406. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
