

From granuloma to fibrosis: sarcoidosis associated pulmonary fibrosis
- PMID: 27379967
- PMCID: PMC5532138
- DOI: 10.1097/MCP.0000000000000301
From granuloma to fibrosis: sarcoidosis associated pulmonary fibrosis
Abstract
Purpose of review: Up to twenty percent of patients with sarcoidosis develop pulmonary fibrosis, transforming an often benign disease into a highly morbid and potentially fatal one. We highlight the fibrotic pulmonary sarcoidosis phenotype as an area of intense clinical and translational investigation, review recent developments in treatment, and provide a roadmap for future research in sarcoidosis associated pulmonary fibrosis.
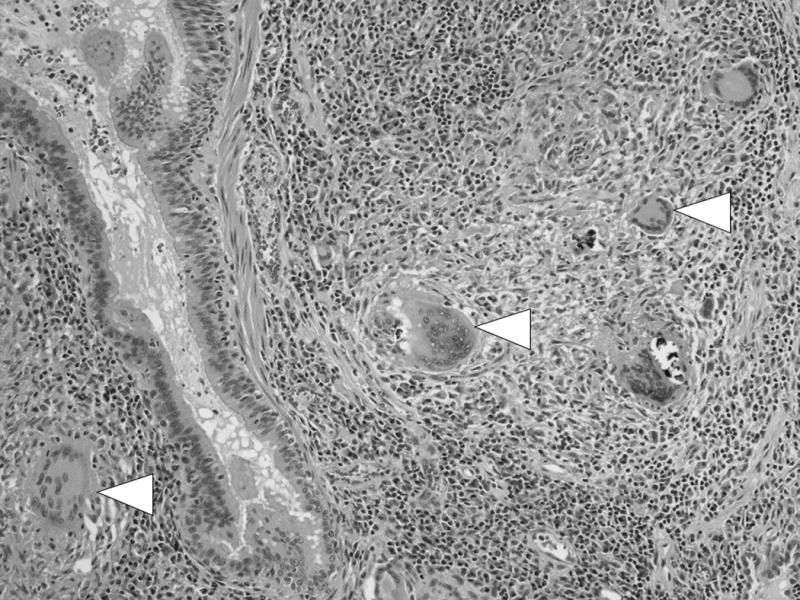
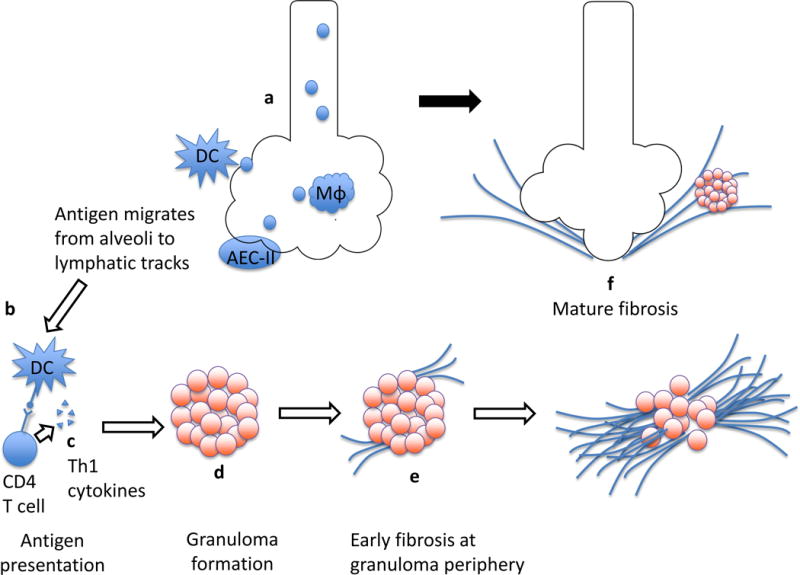
Recent findings: Granulomatous inflammation in a lymphatic distribution is the hallmark finding of pulmonary sarcoidosis and the nidus for fibrosis. Recent research demonstrates that fibrotic sarcoidosis begins in the setting of persistent, uncontrolled inflammation, and is aided by pro-fibrotic genetic features and immune responses. Comparison to other fibrotic lung diseases also reveals key features that inform our understanding of common pathways in fibrosis.
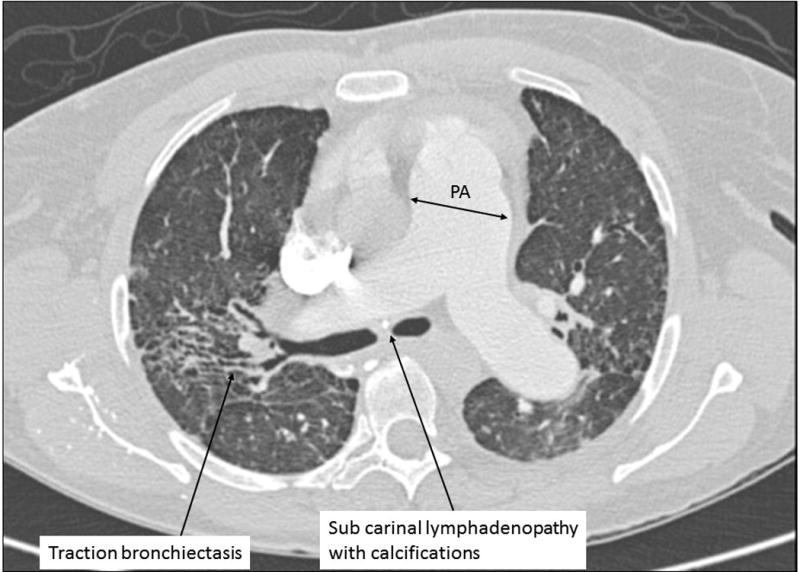
Summary: Understanding the mechanisms of fibrotic transformation in sarcoidosis enhances clinical care and facilitates development of novel therapeutic options. The impact of these findings in fibrotic sarcoidosis may be amplified through application to other interstitial lung diseases marked by inflammatory to fibrotic transformation. Important aspects of clinical management of fibrotic sarcoidosis include surveillance for co-morbidities, such as pulmonary hypertension, airway disease, and infection, and assessment for pulmonary disease activity that may benefit from immunosuppression.
Conflict of interest statement
The authors have no relevant conflicts of interest or sources of funding.
Figures
References
-
- Rosen Y. Pathology of sarcoidosis. Semin Respir Crit Care Med. 2007;28(1):36–52. - PubMed
-
- Grunewald J, Kaiser Y, Ostadkarampour M, Rivera NV, Vezzi F, Lotstedt B, et al. T-cell receptor-HLA-DRB1 associations suggest specific antigens in pulmonary sarcoidosis. Eur Respir J. 2016;47(3):898–909. - PubMed
-
- Kouranos V, Jacob J, Wells AU. Severe Sarcoidosis. Clin Chest Med. 2015;36(4):715–26. - PubMed
-
- Valeyre D, Prasse A, Nunes H, Uzunhan Y, Brillet P-Y, Müller-Quernheim J. Sarcoidosis. The Lancet. 2014;383(9923):1155–67. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
