

Updates in the management of brain metastases
- PMID: 27382120
- PMCID: PMC4933491
- DOI: 10.1093/neuonc/now127
Updates in the management of brain metastases
Abstract
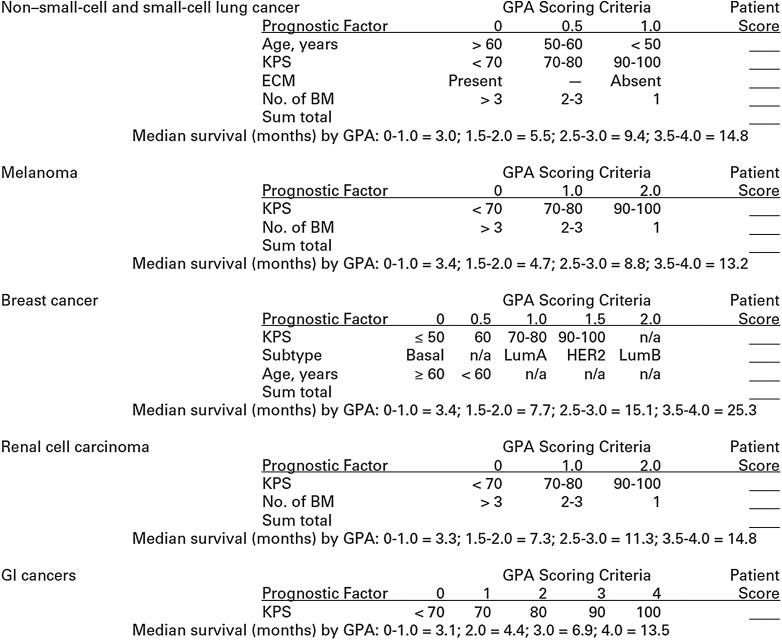
The clinical management/understanding of brain metastases (BM) has changed substantially in the last 5 years, with key advances and clinical trials highlighted in this review. Several of these changes stem from improvements in systemic therapy, which have led to better systemic control and longer overall patient survival, associated with increased time at risk for developing BM. Development of systemic therapies capable of preventing BM and controlling both intracranial and extracranial disease once BM are diagnosed is paramount. The increase in use of stereotactic radiosurgery alone for many patients with multiple BM is an outgrowth of the desire to employ treatments focused on local control while minimizing cognitive effects associated with whole brain radiotherapy. Complications from BM and their treatment must be considered in comprehensive patient management, especially with greater awareness that the majority of patients do not die from their BM. Being aware of significant heterogeneity in prognosis and therapeutic options for patients with BM is crucial for appropriate management, with greater attention to developing individual patient treatment plans based on predicted outcomes; in this context, recent prognostic models of survival have been extensively revised to incorporate molecular markers unique to different primary cancers.
Keywords: brain metastases; chemotherapy; stereotactic radiosurgery; surgery; whole brain radiation.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Gavrilovic IT, Posner JB. Brain metastases: epidemiology and pathophysiology. J Neurooncol. 2005;75(1):5–14. - PubMed
-
- Sawaya R, Bindal R, Lang F et al. . Metastatic brain tumors. In: Kaye A, Laws E, eds. Brain tumors: an encyclopedic approach. 2nd ed London: Churchill Livingstone; 2001:999–1026.
-
- Fox BD, Cheung VJ, Patel AJ et al. . Epidemiology of metastatic brain tumors. Neurosurg Clin N Am. 2011;22(1):1–6. - PubMed
-
- Barnholtz-Sloan JS, Sloan AE, Davis FG et al. . Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol. 2004;22(14):2865–2872. - PubMed
-
- Lin NU, Winer EP. Brain metastases: the HER2 paradigm. Clin Cancer Res. 2007;13(6):1648–1655. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
