

Twenty-Eight-Day Mortality of Blunt Traumatic Brain Injury and Co-Injuries Requiring Mechanical Ventilation
- PMID: 27383217
- PMCID: PMC5588441
- DOI: 10.1159/000447566
Twenty-Eight-Day Mortality of Blunt Traumatic Brain Injury and Co-Injuries Requiring Mechanical Ventilation
Abstract
Objective: This paper aims to assess the impact of co-injuries and consequent emergency surgical interventions and nosocomial pneumonia on the 28-day mortality of patients with severe traumatic brain injuries (TBIs).
Subjects and methods: One hundred and seventy-seven patients with TBI admitted to the emergency trauma intensive care unit at the Clinical Center of Serbia for more than 48 h were studied over a 1-year period. On admission, the Glasgow Coma Scale (GCS), Injury Severity Score (ISS) and Acute Physiology and Chronic Health Evaluation II score (APACHE II) were calculated. At admission, an isolated TBI was recorded in 45 of the patients, while 44 had three or more co-injuries.
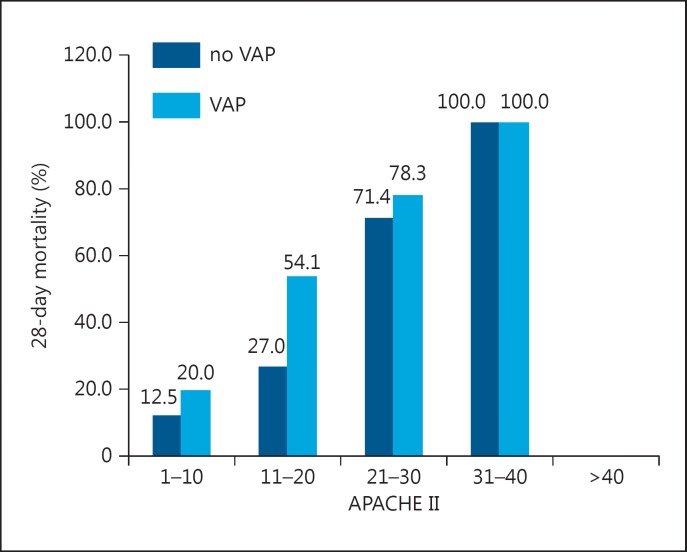
Results: Of the 177 patients, 78 (44.1%) died by the end of the 28-day follow-up period. They had a significantly higher ISS score (25 vs. 20; p = 0.024) and more severe head (p = 0.034) and chest (p = 0.013) injuries compared to those who survived. Nonsurvivors had spent more days on mechanical ventilation (9.5 vs. 8; p = 0.041) and had a significantly higher incidence of ventilator-associated pneumonia (VAP) than survivors (67.9 vs. 40.4%; p < 0.001). A high Rotterdam CT score (OR 2.062; p < 0.001) and a high APACHE II score (OR 1.219; p < 0.001) were identified as independent predictors of early TBI-related mortality.
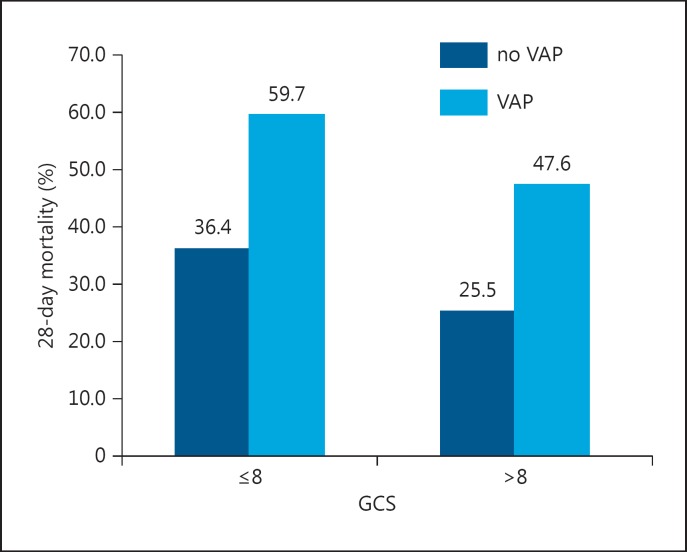
Conclusion: Patients who had TBI with a high Rotterdam score and a high APACHE II score were at higher risk of 28-day mortality. VAP was a very common complication of TBI and was associated with an early death and higher mortality in the subgroup of patients with a GCS ≤8.
© 2016 S. Karger AG, Basel.
Figures
References
-
- Kristiansen T, Lossius HM, Rehn M. Epidemiology of trauma: a population-based study of geographical risk factors for injury deaths in the working-age population of Norway. Injury. 2014;45:23–30. - PubMed
-
- McGarry LJ, Thompson D, Millham FH, et al. Outcomes and costs of acute treatment of traumatic brain injury. J Trauma. 2002;53:1152–1159. - PubMed
-
- Masson F, Thicoipe M, Aye P, et al. Epidemiology of severe brain injuries: a prospective population-based study. J Trauma. 2001;51:481–489. - PubMed
-
- Roozenbeek B, Maas AI, Menon DK. Changing patterns in the epidemiology of traumatic brain injury. Nat Rev Neurol. 2013;9:231–236. - PubMed
-
- Maas AI, Stocchetti N, Bullock R. Moderate and severe traumatic brain injury in adults. Lancet Neurol. 2008;7:728–741. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
