

The Effect of Antiretroviral Treatment on Health Care Utilization in Rural South Africa: A Population-Based Cohort Study
- PMID: 27384178
- PMCID: PMC4934780
- DOI: 10.1371/journal.pone.0158015
The Effect of Antiretroviral Treatment on Health Care Utilization in Rural South Africa: A Population-Based Cohort Study
Abstract
Background: The effect of the rapid scale-up of vertical antiretroviral treatment (ART) programs for HIV in sub-Saharan Africa on the overall health system is under intense debate. Some have argued that these programs have reduced access for people suffering from diseases unrelated to HIV because ART programs have drained human and physical resources from other parts of the health system; others have claimed that the investments through ART programs have strengthened the general health system and the population health impacts of ART have freed up health care capacity for the treatment of diseases that are not related to HIV. To establish the population-level impact of ART programs on health care utilization in the public-sector health system, we compared trends in health care utilization among HIV-infected people receiving and not receiving ART with HIV-uninfected people during a period of rapid ART scale-up.
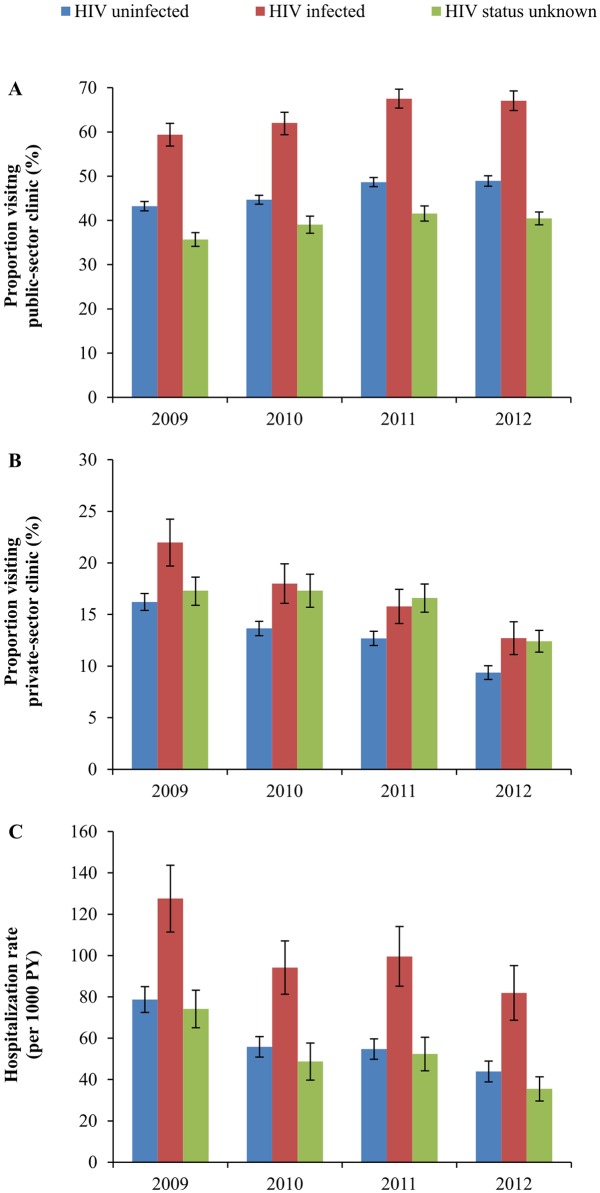
Methods and findings: We used data from the Wellcome Trust Africa Centre for Population Health, which annually elicited information on health care utilization from all surveillance participants over the period 2009-2012 (N = 32,319). We determined trends in hospitalization, and public-sector and private-sector primary health care (PHC) clinic visits for HIV-infected and -uninfected people over a time period of rapid ART scale-up (2009-2012) in this community. We regressed health care utilization on HIV status and ART status in different calendar years, controlling for sex, age, and area of residence. The proportion of people who reported to have visited a public-sector primary health care (PHC) clinic in the last 6 months increased significantly over the period 2009-2012, for both HIV-infected people (from 59% to 67%; p<0.001), and HIV-uninfected people (from 41% to 47%; p<0.001). In contrast, the proportion of HIV-infected people visiting a private-sector PHC clinic declined from 22% to 12% (p<0.001) and hospitalization rates declined from 128 to 82 per 1000 PY (p<0.001). For HIV-uninfected people, the proportion visiting a private-sector PHC clinic declined from 16% to 9%, and hospitalization rates declined from 78 to 44 per 1000 PY (p<0.001). After controlling for potential confounding factors, all trends remained of similar magnitude and significance.
Conclusions: Our results indicate that the ART scale-up in this high HIV prevalence community has shifted health care utilization from hospitals and private-sector primary care to public-sector primary care. Remarkably, this shift is observed for both HIV-infected and -uninfected populations, supporting and extending hypotheses of 'therapeutic citizenship' whereby HIV-infected patients receiving ART facilitate primary care access for family and community members. One explanation of our findings is that ART has improved the capacity or quality of primary care in this community and, as a consequence, increasingly met overall health care needs at the primary care level rather than at the secondary level. Future research needs to confirm this causal interpretation of our findings using qualitative work to understand causal mechanisms or quasi-experimental quantitative studies to increase the strength of causal inference.
Conflict of interest statement
Figures
Similar articles
-
HIV status and participation in HIV surveillance in the era of antiretroviral treatment: a study of linked population-based and clinical data in rural South Africa.Trop Med Int Health. 2012 Aug;17(8):e103-10. doi: 10.1111/j.1365-3156.2012.02928.x. Trop Med Int Health. 2012. PMID: 22943374 Free PMC article.
-
Use of antiretroviral therapy in households and risk of HIV acquisition in rural KwaZulu-Natal, South Africa, 2004–12: a prospective cohort study.Lancet Glob Health. 2014 Apr;2(4):e209-15. doi: 10.1016/S2214-109X(14)70018-X. Lancet Glob Health. 2014. PMID: 24782953 Free PMC article.
-
Prevalence, incidence, predictors, treatment, and control of hypertension among HIV-positive adults on antiretroviral treatment in public sector treatment programs in South Africa.PLoS One. 2018 Oct 3;13(10):e0204020. doi: 10.1371/journal.pone.0204020. eCollection 2018. PLoS One. 2018. PMID: 30281618 Free PMC article.
-
Effect of HIV status and antiretroviral treatment on treatment outcomes of tuberculosis patients in a rural primary healthcare clinic in South Africa.PLoS One. 2022 Oct 12;17(10):e0274549. doi: 10.1371/journal.pone.0274549. eCollection 2022. PLoS One. 2022. PMID: 36223365 Free PMC article. Review.
-
Implementing antiretroviral therapy in rural communities: the Lusikisiki model of decentralized HIV/AIDS care.J Infect Dis. 2007 Dec 1;196 Suppl 3:S464-8. doi: 10.1086/521114. J Infect Dis. 2007. PMID: 18181695 Review.
Cited by
-
"Our Tradition Our Enemy": A Qualitative Study of Barriers to Women's HIV Care in Jimma, Southwest Ethiopia.Int J Environ Res Public Health. 2020 Jan 29;17(3):833. doi: 10.3390/ijerph17030833. Int J Environ Res Public Health. 2020. PMID: 32013114 Free PMC article.
-
Effect of ART scale-up and female migration intensity on risk of HIV acquisition: results from a population-based cohort in KwaZulu-Natal, South Africa.BMC Public Health. 2019 Feb 14;19(1):196. doi: 10.1186/s12889-019-6494-x. BMC Public Health. 2019. PMID: 30764786 Free PMC article.
-
Human Resources for Treating HIV/AIDS: Are the Preventive Effects of Antiretroviral Treatment a Game Changer?PLoS One. 2016 Oct 7;11(10):e0163960. doi: 10.1371/journal.pone.0163960. eCollection 2016. PLoS One. 2016. PMID: 27716813 Free PMC article.
-
Hospitalization rates, length of stay and in-hospital mortality in a cohort of HIV infected patients from Rio de Janeiro, Brazil.Braz J Infect Dis. 2017 Mar-Apr;21(2):190-195. doi: 10.1016/j.bjid.2016.10.007. Epub 2016 Dec 3. Braz J Infect Dis. 2017. PMID: 27918889 Free PMC article.
-
Interventions to improve primary healthcare in rural settings: A scoping review.PLoS One. 2024 Jul 11;19(7):e0305516. doi: 10.1371/journal.pone.0305516. eCollection 2024. PLoS One. 2024. PMID: 38990801 Free PMC article.
References
-
- UNAIDS (2014) Report on the Global AIDS epidemic 2014. Geneva: UNAIDS.
-
- Atun R, Bennett S, Duran A (2008) When do vertical (stand-alone) programmes have a place in health systems? Geneva: World Health Organization.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
