

Circulating tumor DNA analysis detects minimal residual disease and predicts recurrence in patients with stage II colon cancer
- PMID: 27384348
- PMCID: PMC5346159
- DOI: 10.1126/scitranslmed.aaf6219
Circulating tumor DNA analysis detects minimal residual disease and predicts recurrence in patients with stage II colon cancer
Abstract
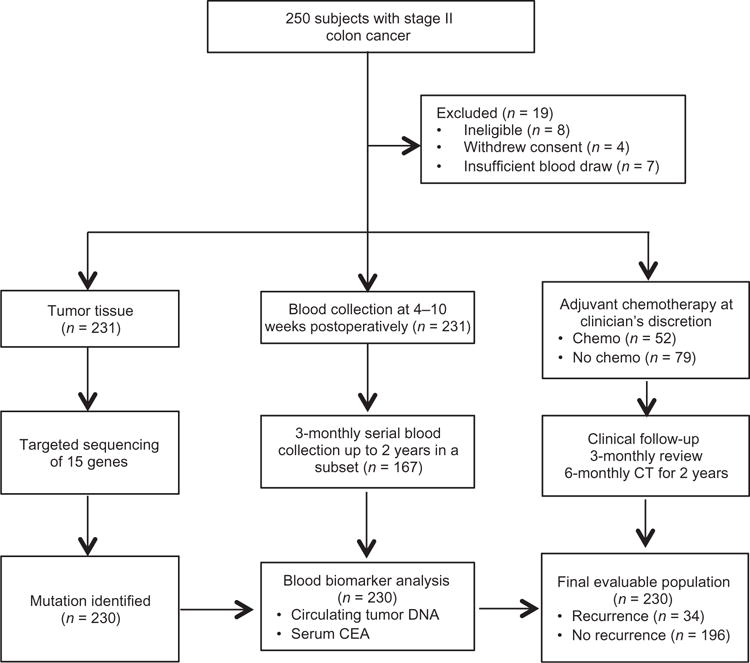
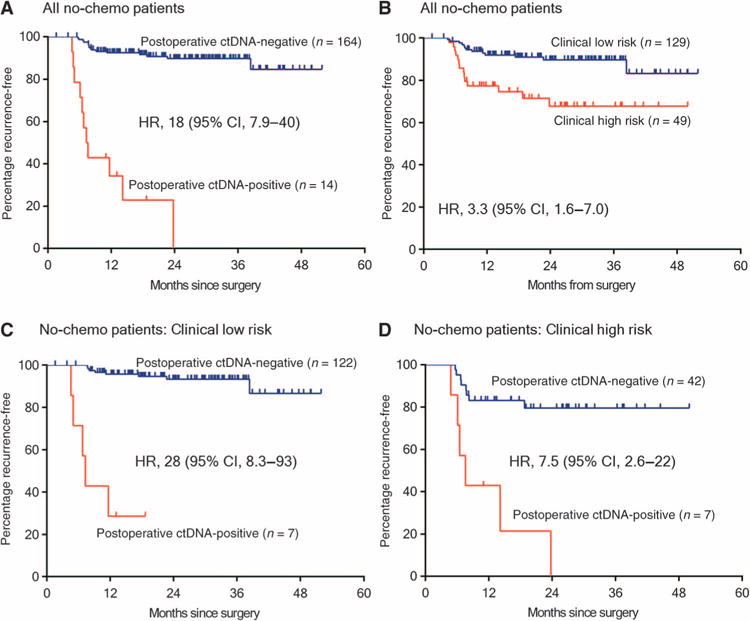
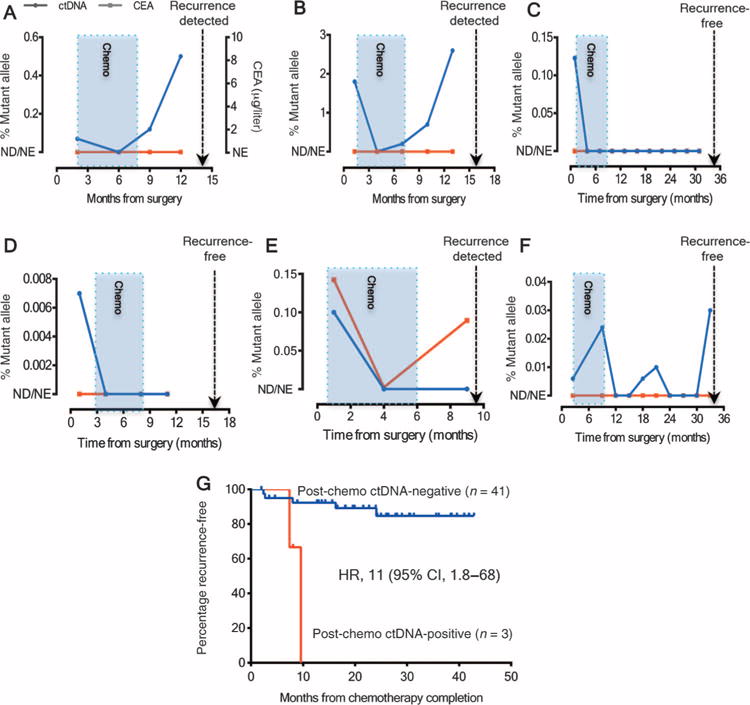
Detection of circulating tumor DNA (ctDNA) after resection of stage II colon cancer may identify patients at the highest risk of recurrence and help inform adjuvant treatment decisions. We used massively parallel sequencing-based assays to evaluate the ability of ctDNA to detect minimal residual disease in 1046 plasma samples from a prospective cohort of 230 patients with resected stage II colon cancer. In patients not treated with adjuvant chemotherapy, ctDNA was detected postoperatively in 14 of 178 (7.9%) patients, 11 (79%) of whom had recurred at a median follow-up of 27 months; recurrence occurred in only 16 (9.8 %) of 164 patients with negative ctDNA [hazard ratio (HR), 18; 95% confidence interval (CI), 7.9 to 40; P < 0.001]. In patients treated with chemotherapy, the presence of ctDNA after completion of chemotherapy was also associated with an inferior recurrence-free survival (HR, 11; 95% CI, 1.8 to 68; P = 0.001). ctDNA detection after stage II colon cancer resection provides direct evidence of residual disease and identifies patients at very high risk of recurrence.
Copyright © 2016, American Association for the Advancement of Science.
Conflict of interest statement
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. - PubMed
-
- Edge S, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC Cancer Staging Manual. Springer; New York: 2010. p. 648.
-
- Dukes CE. The classification of cancer of the rectum. J Pathol Bacteriol. 1932;35:323–332.
-
- Quah H-M, Chou JF, Gonen M, Shia J, Schrag D, Landmann RG, Guillem JG, Paty PB, Temple LK, Wong WD, Weiser MR. Identification of patients with high-risk stage II colon cancer for adjuvant therapy. Dis Colon Rectum. 2008;51:503–507. - PubMed
-
- Niedzwiecki D, Bertagnolli MM, Warren RS, Compton CC, Kemeny NE, Benson AB, III, Eckhardt SG, Alberts S, Porjosh GN, Kerr DJ, Fields A, Rougier P, Pipas JM, Schwartz JH, Atkins J, O’Rourke M, Perry MC, Goldberg RM, Mayer RJ, Colacchio TA. Documenting the natural history of patients with resected stage II adenocarcinoma of the colon after random assignment to adjuvant treatment with edrecolomab or observation: Results from CALGB 9581. J Clin Oncol. 2011;29:3146–3152. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
