

Fibrobronchoscopic cryosurgery for secondary malignant tumors of the trachea and main bronchi
- PMID: 27385989
- PMCID: PMC4930966
- DOI: 10.1111/1759-7714.12337
Fibrobronchoscopic cryosurgery for secondary malignant tumors of the trachea and main bronchi
Abstract
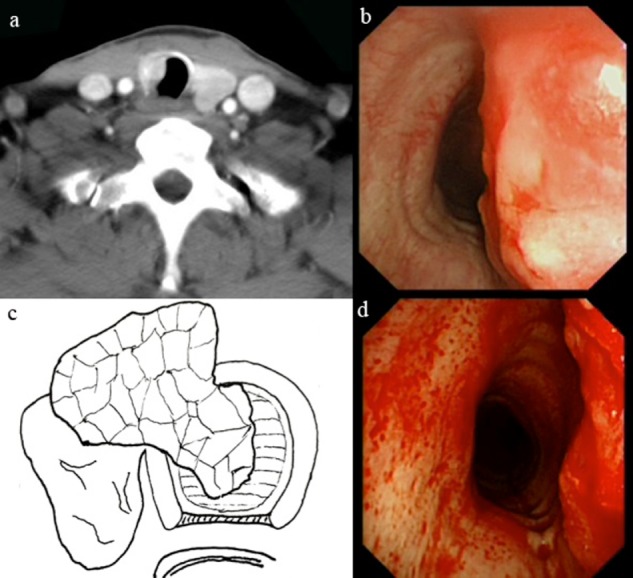
Background: Patients with secondary malignant tracheal and main bronchial tumors may suffer severe symptoms as a result of major airway obstruction. Curative surgical resection is usually not suitable because of the presence of metastatic disease and poor performance status. In this study, the use of bronchoscopic cryosurgery to reopen the airway is analyzed.
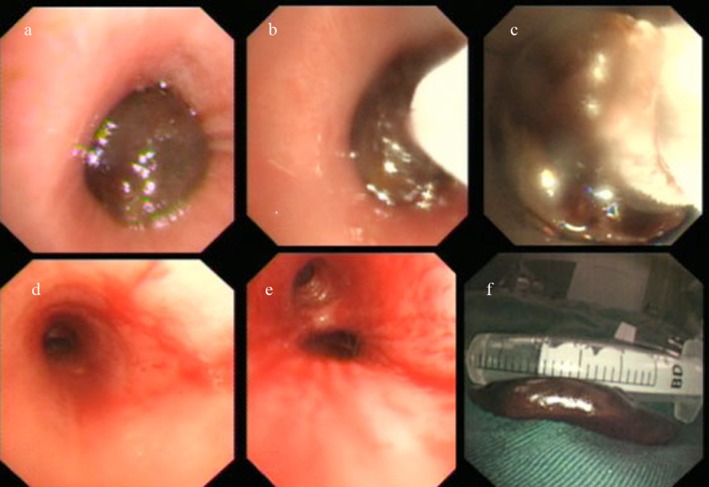
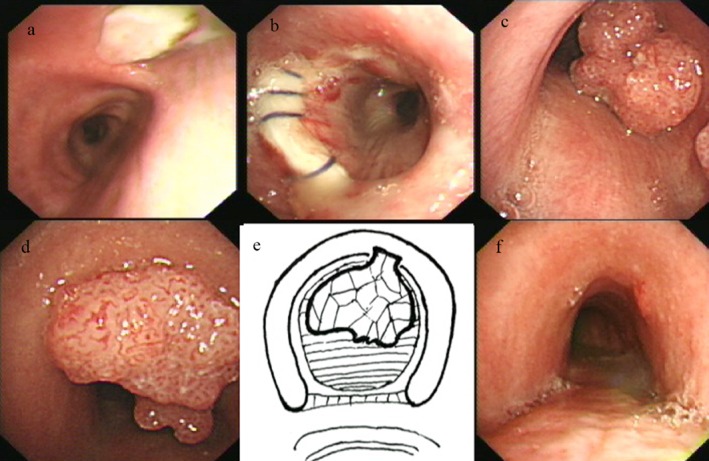
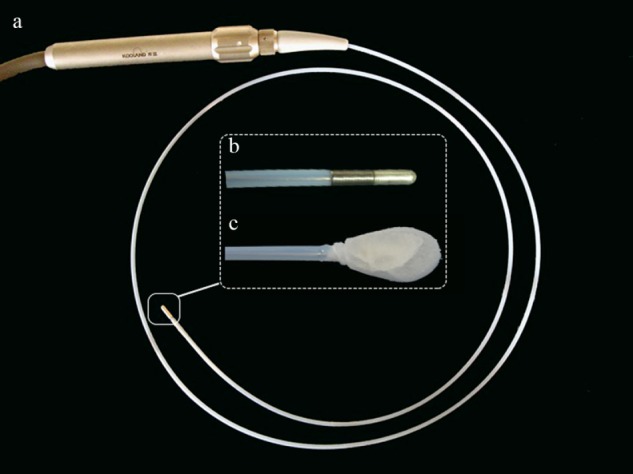
Methods: The clinical records of 37 patients who experienced secondary maglinancies from December 2001 to January 2013 were retrospectively reviewed. Low temperature cryotherapy (-50°C to -70°C) was delivered to the central part of the tumor by cryoprobe for four to six minutes causing destruction of the tumor mass (Cryo-melt method). Subsequently, the edge of the tumor was frozen for 30 seconds to two minutes, followed by piecemeal removal of the frozen tumor tissue (Cryo-resection method).
Results: The endpoints of the study were degree of symptomatic improvement and survival. The rates of dramatic and partial symptomatic alleviation were 57.1% and 28.6%, respectively, there were no intraoperative deaths, and median survival was 16.0 months. Prolonged survival was significantly correlated to age (under 60 years of age 22.2% vs. over 60 100%, P = 0.011), tumor location (main bronchi 0% vs. trachea 77.8%, P = 0.003), and cryorecanalization times (once 33.3% vs. twice or more 80.0%, P = 0.037).
Conclusion: Bronchoscopic cryorecanalization is a safe, effective, non-invasive choice for improving the symptoms of malignant airway obstruction. In addition to achieving local-regional control, the technique may also contribute to improved survival.
Keywords: Airway obstruction; bronchoscopy; cryosurgery; secondary tracheobronchial tumors.
Figures
Similar articles
-
[Fibro-bronchoscopic cryosurgery for unresectable endobronchial tumors].Zhongguo Fei Ai Za Zhi. 2014 Jul 20;17(7):545-9. doi: 10.3779/j.issn.1009-3419.2014.07.08. Zhongguo Fei Ai Za Zhi. 2014. PMID: 25034584 Free PMC article. Chinese.
-
Cryorecanalization: a new approach for the immediate management of acute airway obstruction.J Thorac Cardiovasc Surg. 2004 May;127(5):1427-31. doi: 10.1016/j.jtcvs.2003.12.032. J Thorac Cardiovasc Surg. 2004. PMID: 15116003
-
Cryosurgery for malignant endobronchial tumors: analysis of outcome.Chest. 2005 Jun;127(6):2007-14. doi: 10.1378/chest.127.6.2007. Chest. 2005. PMID: 15947313
-
Bronchoscopic preparation for airway resection.Chest Surg Clin N Am. 2001 Nov;11(4):735-48. Chest Surg Clin N Am. 2001. PMID: 11780293 Review.
-
Tracheostenosis and bronchial abnormalities associated with pulmonary artery sling.Ann Otol Rhinol Laryngol. 1976 Sep-Oct;85(5 Pt.1):582-90. doi: 10.1177/000348947608500504. Ann Otol Rhinol Laryngol. 1976. PMID: 791050 Review.
Cited by
-
Tuberculous tracheobronchial stenosis: avoiding resection-when less is more.J Thorac Dis. 2017 Sep;9(9):E779-E782. doi: 10.21037/jtd.2017.08.104. J Thorac Dis. 2017. PMID: 29221342 Free PMC article.
-
Secondary tracheal tumors: a systematic review.Ann Cardiothorac Surg. 2018 Mar;7(2):183-196. doi: 10.21037/acs.2018.02.01. Ann Cardiothorac Surg. 2018. PMID: 29707496 Free PMC article. Review.
-
Central airway tumors: interventional bronchoscopy in diagnosis and management.J Thorac Dis. 2016 Oct;8(10):E1168-E1176. doi: 10.21037/jtd.2016.10.101. J Thorac Dis. 2016. PMID: 27867582 Free PMC article. Review.
-
Comparative study of cryorecanalisation and cryoablation using flexible bronchoscopy for the treatment of endobronchial tuberculosis.Updates Surg. 2025 Apr;77(2):559-566. doi: 10.1007/s13304-024-02031-x. Epub 2024 Dec 13. Updates Surg. 2025. PMID: 39671075 Clinical Trial.
-
Bronchoscopic cryosurgery for metastatic tumor causing central airway obstruction: A case report.Medicine (Baltimore). 2019 Mar;98(9):e14635. doi: 10.1097/MD.0000000000014635. Medicine (Baltimore). 2019. PMID: 30817581 Free PMC article.
References
-
- Pass HI, Donigtom JS. Metastatic cancer to the lung In: DeVita VT Jr, Hellman S, Rosenberg SA. (eds). Cancer: Principles and Practice of Oncology. Lippincott Rowen, Philadelphia, PA: 1997; 2536–2550.
-
- Maiwand MO, Homasson JP. Cryotherapy for tracheobronchial disorders. (Published erratum appears in Clin Chest Med 1995; 16: ix) Clin Chest Med 1995; 16: 427–443. - PubMed
-
- Arnott J. On the Treatment of Cancer by Regulated Application of Anaesthetic Temperature. J Churchill, London; 1851.
-
- Cooper IS, Lee AS. Cryostatic congelation: A system for producing a limited, controlled region of cooling or freezing of biologic tissues. J Nerv Ment Dis 1961; 133: 259–263. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
