

The utility of the aortic dissection team: outcomes and insights after a decade of experience
- PMID: 27386406
- PMCID: PMC4893530
- DOI: 10.21037/acs.2016.05.12
The utility of the aortic dissection team: outcomes and insights after a decade of experience
Abstract
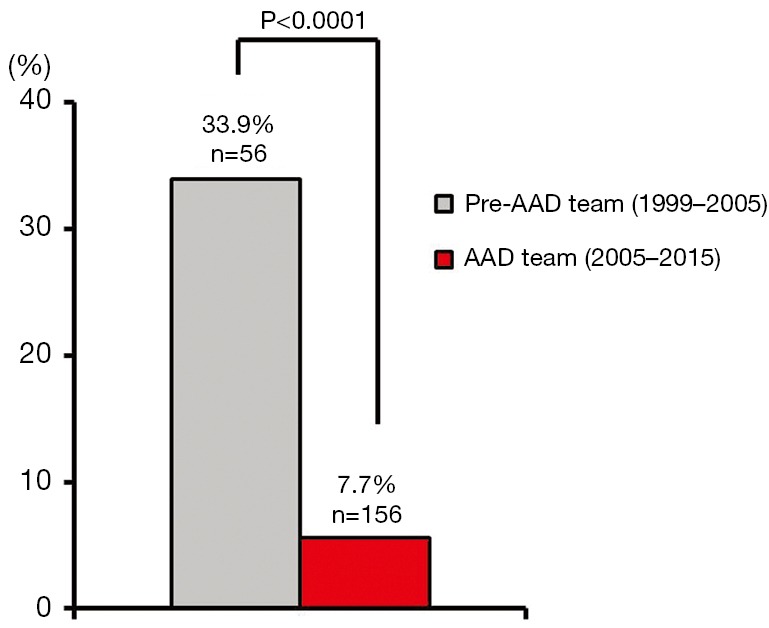
Background: Mortality rates following acute type A aortic dissection (ATAAD) repair are reduced when operations are performed by a high-volume acute aortic dissection (AAD) team, leading to efforts to centralize ATAAD care. Here, we describe our experience with ATAAD repair by our AAD team over the last 10 years, with a focus on patient selection, transfer protocols, operative approach, and volume trends over time.
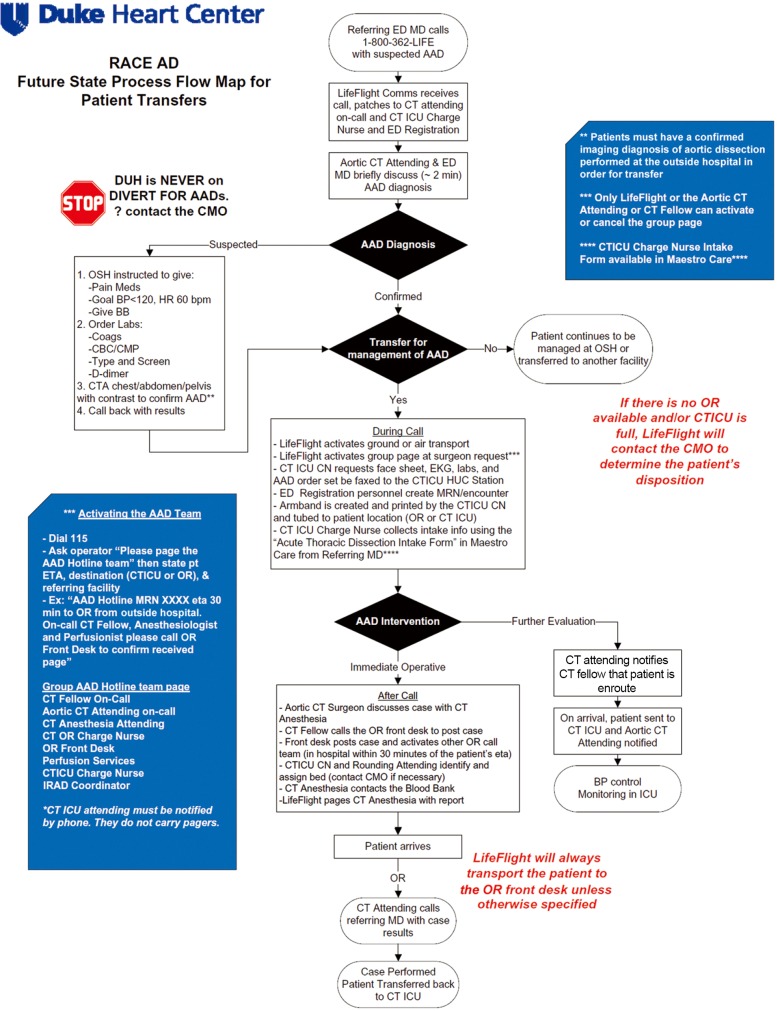
Methods: An AAD team was implemented at our institution in 2005, with dedicated high-volume AAD surgeons, a multidisciplinary approach to thoracic aortic disease management, and a standardized protocol for ATAAD repair. Further process improvements were made in 2013 to facilitate the rapid transfer of ATAAD patients to our institution using stream-lined triage, diagnostic, and transfer protocols for patients with suspected ATAAD (RACE-AD protocol). Volume trends and outcomes were assessed longitudinally over this period.
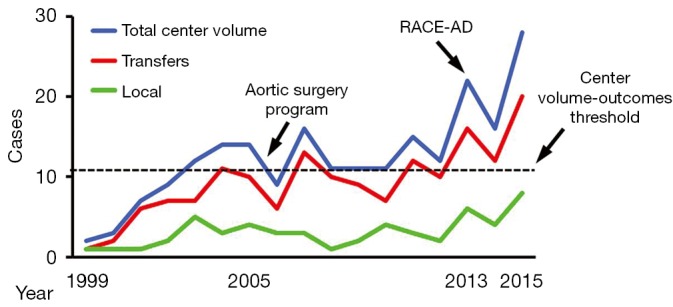
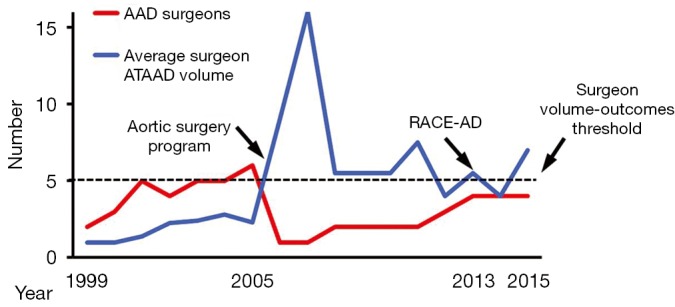
Results: Institutional ATAAD repair volume remained constant at 12±2 cases per year from 2005-2013, but increased nearly two-fold to 22±6 cases per year (P=0.004) from 2013-2015 following implementation of the RACE-AD protocol. To accommodate this increased volume, two additional surgeons were added to the AAD team. Surgeon ATAAD repair volume was unchanged over the 10-year interval (7.9±3.9 cases per year from 2005-2013 versus 5.5±1.5 cases per year from 2013-2015; P=0.36), and all AAD team surgeons consistently met or exceeded the high-volume surgeon threshold of 5 ATAAD repairs per year. Thirty-day/in-hospital mortality rates of less than 10% were maintained over the study period.
Conclusions: Centralization of ATAAD care has begun to occur at our center, with maintenance of low mortality rates for ATAAD repair. These data confirm a net positive impact on regional ATAAD outcomes through transfer of patients to a high-volume center with dedicated AAD surgeons.
Keywords: Aorta; dissection; process improvement.
Conflict of interest statement
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous