

Surgical management of acute type A aortic dissection: branch-first arch replacement with total aortic repair
- PMID: 27386413
- PMCID: PMC4893537
- DOI: 10.21037/acs.2016.05.11
Surgical management of acute type A aortic dissection: branch-first arch replacement with total aortic repair
Abstract
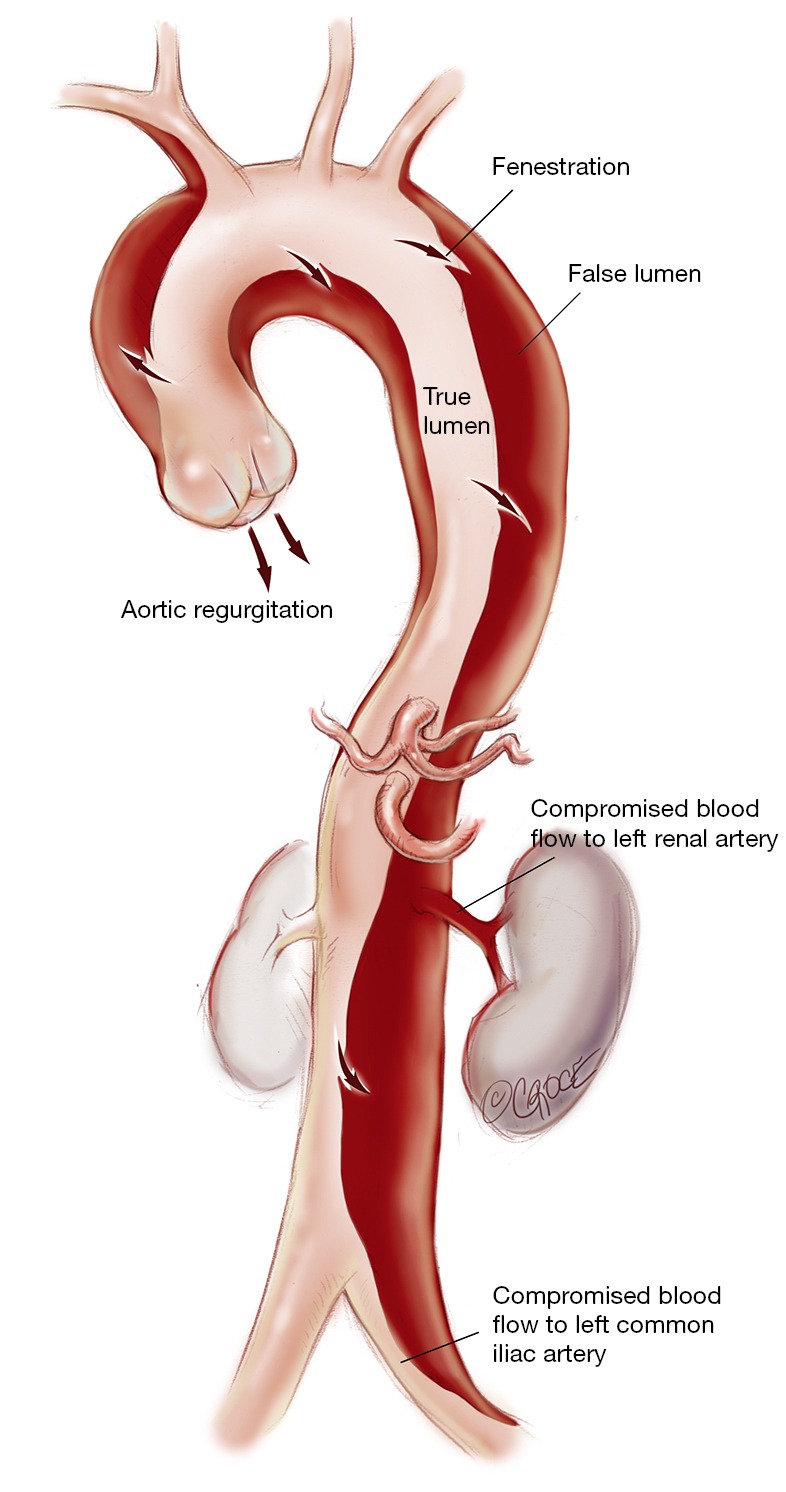
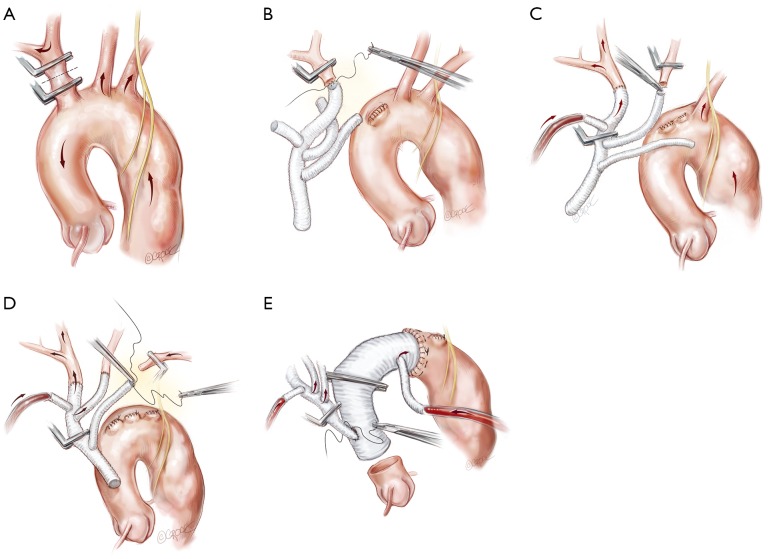
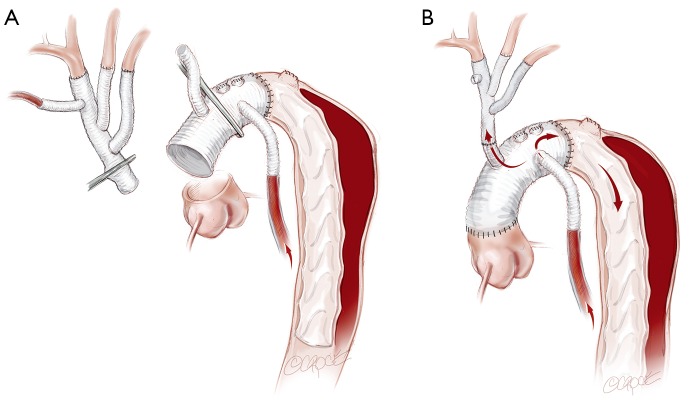
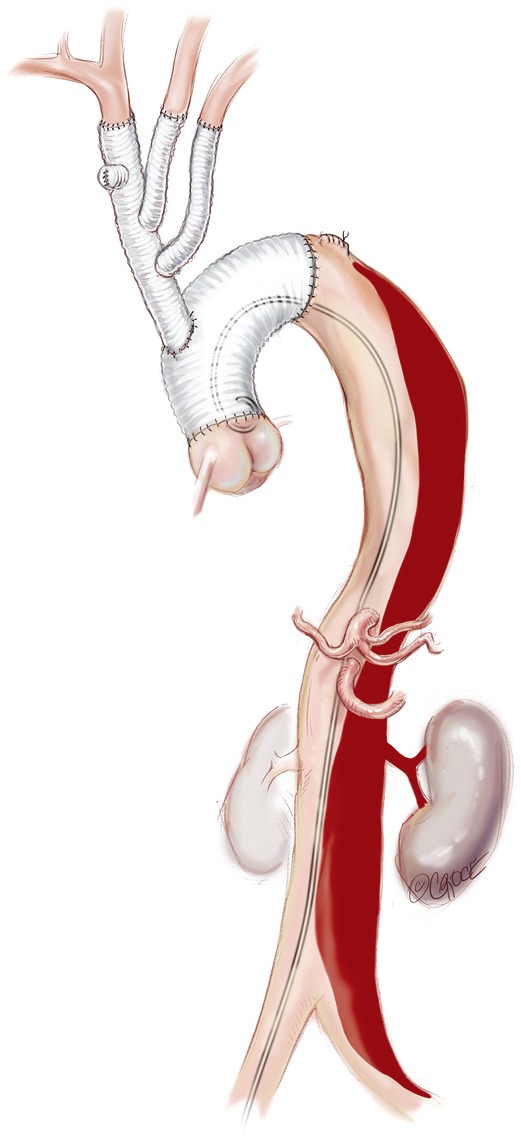
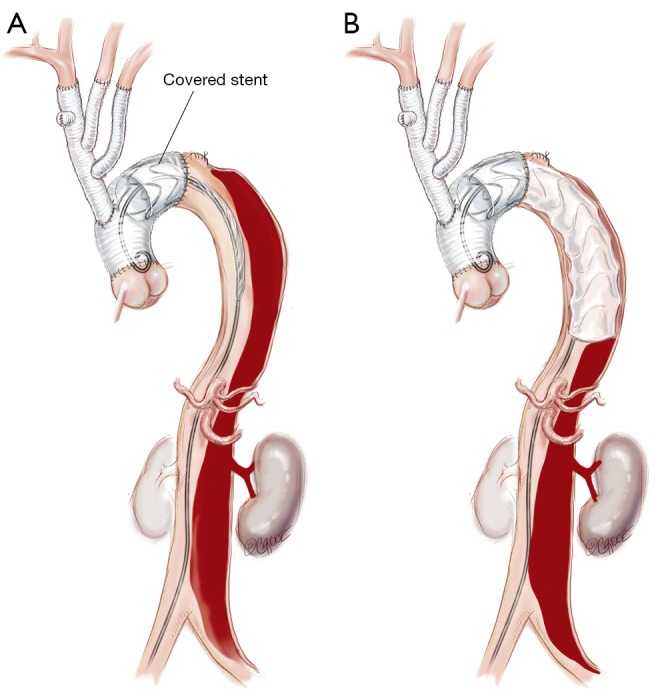
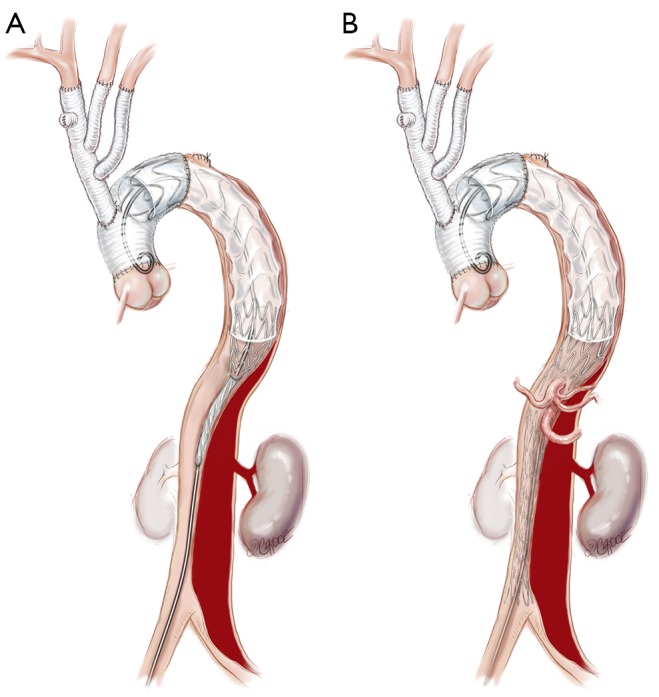
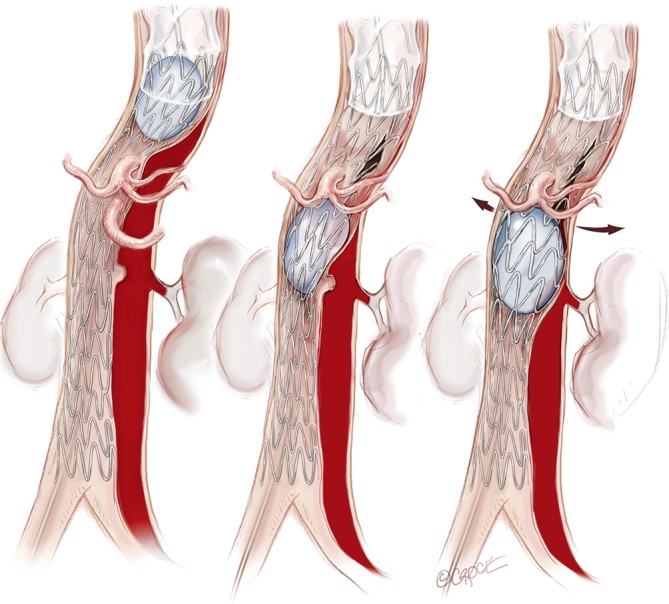
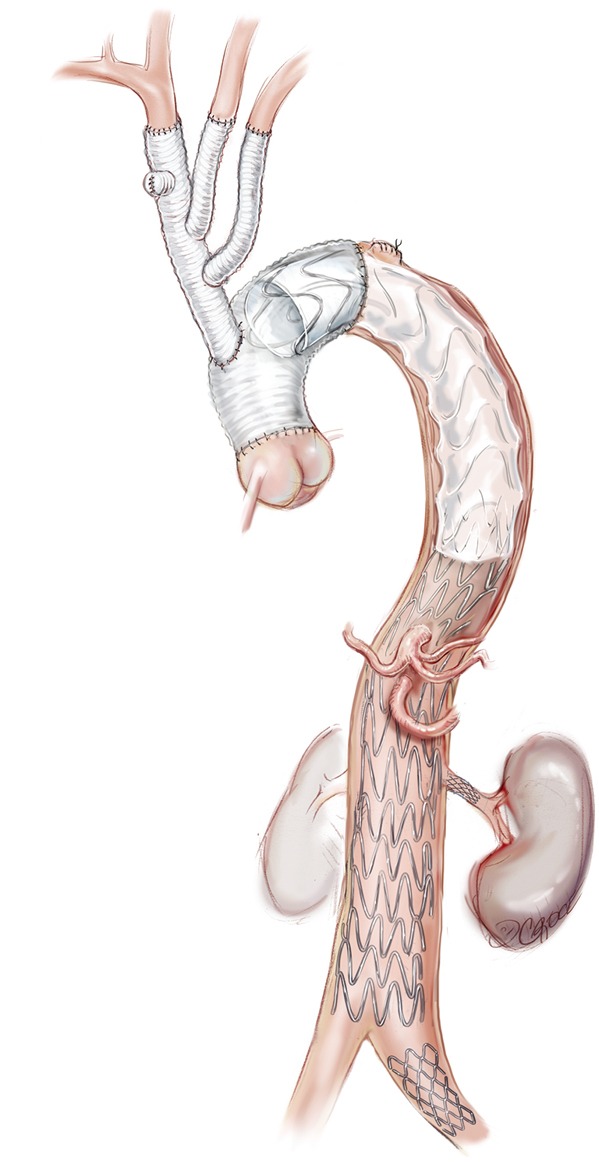
Acute type A dissection (ATAAD) remains a morbid condition with reported surgical mortality as high as 25%. We describe our surgical approach to ATAAD and discuss the indications for adjunct techniques such as the frozen elephant trunk or complete aortic repair with endovascular methods. Arch replacement using the "branch-first technique" allows for complete root, ascending aorta, and arch replacement. A long landing zone is created for proximal endografting with a covered stent. Balloon-assisted intimal disruption and bare metal stenting of all residual dissected aorta to the level of the aortic bifurcation is then performed to obliterate the false lumen (FL) and achieve single true lumen (TL) flow. Additional branch vessel stenting is performed as required.
Keywords: Aorta; dissection; endovascular techniques.
Conflict of interest statement
Figures
Similar articles
-
Aortic remodeling, reintervention, and survival after zone 0 arch repair with frozen elephant trunks for acute type A aortic dissection: Midterm results.JTCVS Tech. 2022 May 31;14:29-38. doi: 10.1016/j.xjtc.2022.05.013. eCollection 2022 Aug. JTCVS Tech. 2022. PMID: 35967231 Free PMC article.
-
A case of stent-assisted balloon-induced intimal disruption and relamination of distal remaining aortic dissection after the ascending aorta and aortic arch replacement for acute aortic dissection.Gen Thorac Cardiovasc Surg Cases. 2023 Sep 14;2(1):55. doi: 10.1186/s44215-023-00071-0. Gen Thorac Cardiovasc Surg Cases. 2023. PMID: 39516910 Free PMC article.
-
Trends and controversies in type A aortic surgery in the 21st century: Branch first aortic arch replacement.J Card Surg. 2021 May;36(5):1766-1769. doi: 10.1111/jocs.15037. Epub 2020 Sep 29. J Card Surg. 2021. PMID: 32996210
-
The Management of the Aortic Arch in Type A Aortic Dissection: Replace, Repair with the AMDS, or Leave for Another Day?J Cardiovasc Dev Dis. 2025 Jan 12;12(1):23. doi: 10.3390/jcdd12010023. J Cardiovasc Dev Dis. 2025. PMID: 39852301 Free PMC article. Review.
-
Hybrid aortic arch and frozen elephant trunk reconstruction: bridging the gap between conventional and total endovascular arch repair.Expert Rev Cardiovasc Ther. 2018 Mar;16(3):209-217. doi: 10.1080/14779072.2018.1429913. Epub 2018 Jan 29. Expert Rev Cardiovasc Ther. 2018. PMID: 29343137 Review.
Cited by
-
Mini-access branch-first total arch replacement and frozen elephant trunk procedure.Ann Cardiothorac Surg. 2020 May;9(3):236-243. doi: 10.21037/acs-2020-fet-27. Ann Cardiothorac Surg. 2020. PMID: 32551260 Free PMC article.
-
Total aortic repair for acute type A aortic dissection: a new paradigm.J Vis Surg. 2018 Apr 26;4:79. doi: 10.21037/jovs.2018.04.04. eCollection 2018. J Vis Surg. 2018. PMID: 29780725 Free PMC article.
-
Hybrid Aortic Arch Replacement with Frozen Elephant Trunk (FET) Technique: Surgical Considerations, Pearls, and Pitfalls.J Clin Med. 2024 Nov 22;13(23):7075. doi: 10.3390/jcm13237075. J Clin Med. 2024. PMID: 39685533 Free PMC article. Review.
-
Surgical repair and reconstruction of aortic arch in debakey type I aortic dissection: recent advances and single-center experience in the application of branched stent graft.J Cardiothorac Surg. 2017 Oct 3;12(1):86. doi: 10.1186/s13019-017-0649-6. J Cardiothorac Surg. 2017. PMID: 28974246 Free PMC article. Review.
-
"Branch-First total arch replacement": a valuable alternative to frozen elephant trunk in acute type A aortic dissection?Indian J Thorac Cardiovasc Surg. 2022 Apr;38(Suppl 1):58-63. doi: 10.1007/s12055-021-01279-x. Epub 2021 Nov 25. Indian J Thorac Cardiovasc Surg. 2022. PMID: 35463702 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources