

Detection and Quantification of Differentially Culturable Tubercle Bacteria in Sputum from Patients with Tuberculosis
- PMID: 27387272
- PMCID: PMC5215032
- DOI: 10.1164/rccm.201604-0769OC
Detection and Quantification of Differentially Culturable Tubercle Bacteria in Sputum from Patients with Tuberculosis
Abstract
Rationale: Recent studies suggest that baseline tuberculous sputum comprises a mixture of routinely culturable and differentially culturable tubercle bacteria (DCTB). The latter seems to be drug tolerant and dependent on resuscitation-promoting factors (Rpfs).
Objectives: To further explore this, we assessed sputum from patients with tuberculosis for DCTB and studied the impact of exogenous culture filtrate (CF) supplementation ex vivo.
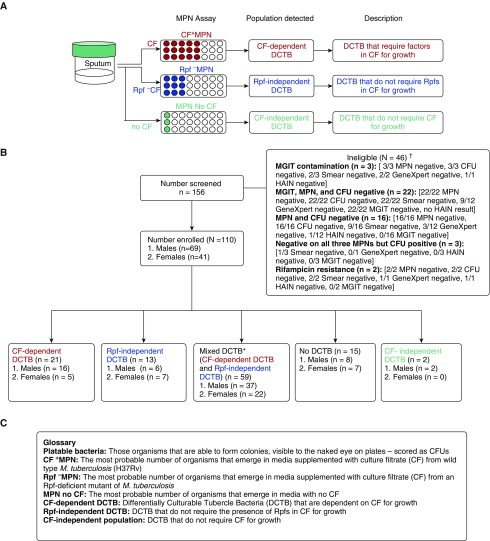
Methods: Sputum samples from adults with tuberculosis and HIV-1 and adults with no HIV-1 were used for most probable number (MPN) assays supplemented with CF and Rpf-deficient CF, to detect CF-dependent and Rpf-independent DCTB, respectively.
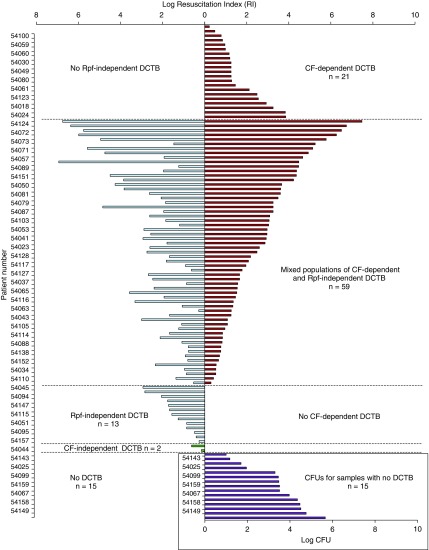
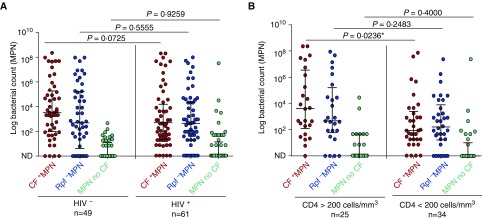
Measurements and main results: In 110 individuals, 19.1% harbored CF-dependent DCTB and no Rpf-independent DCTB. Furthermore, 11.8% yielded Rpf-independent DCTB with no CF-dependent DCTB. In addition, 53.6% displayed both CF-dependent and Rpf-independent DCTB, 1.8% carried CF-independent DCTB, and 13.6% had no DCTB. Sputum from individuals without HIV-1 yielded higher CF-supplemented MPN counts compared with counterparts with HIV-1. Furthermore, individuals with HIV-1 with CD4 counts greater than 200 cells/mm3 displayed higher CF-supplemented MPN counts compared with participants with HIV-1 with CD4 counts less than 200 cells/mm3. CF supplementation allowed for detection of mycobacteria in 34 patients with no culturable bacteria on solid media. Additionally, the use of CF enhanced detection of sputum smear-negative individuals.
Conclusions: These observations demonstrate a novel Rpf-independent DCTB population in sputum and reveal that reduced host immunity is associated with lower prevalence of CF-responsive bacteria. Quantification of DCTB in standard TB diagnosis would be beneficial because these organisms provide a putative biomarker to monitor treatment response and risk of disease recurrence.
Keywords: HIV; culturability; limiting dilution assay; resuscitation-promoting factors; tuberculosis.
Figures
Comment in
-
New Evidence for the Complexity of the Population Structure of Mycobacterium tuberculosis Increases the Diagnostic and Biologic Challenges.Am J Respir Crit Care Med. 2016 Dec 15;194(12):1448-1451. doi: 10.1164/rccm.201607-1431ED. Am J Respir Crit Care Med. 2016. PMID: 27976945 Free PMC article. No abstract available.
References
-
- Zumla A, Kim P, Maeurer M, Schito M. Zero deaths from tuberculosis: progress, reality, and hope. Lancet Infect Dis. 2013;13:285–287. - PubMed
-
- Zumla A, Nahid P, Cole ST. Advances in the development of new tuberculosis drugs and treatment regimens. Nat Rev Drug Discov. 2013;12:388–404. - PubMed
-
- Wallis RS, Kim P, Cole S, Hanna D, Andrade BB, Maeurer M, Schito M, Zumla A. Tuberculosis biomarkers discovery: developments, needs, and challenges. Lancet Infect Dis. 2013;13:362–372. - PubMed
-
- Young M, Mukamolova GV, Kaprelyants AS.Mycobacterial dormancy and its relation to persistence Parish T.editor. Mycobacterium: molecular biology Norwich, UK: Horizon Scientific; 2005265–320.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
