

Evaluation of the FACSPresto, a New Point of Care Device for the Enumeration of CD4% and Absolute CD4+ T Cell Counts in HIV Infection
- PMID: 27388763
- PMCID: PMC4936750
- DOI: 10.1371/journal.pone.0157546
Evaluation of the FACSPresto, a New Point of Care Device for the Enumeration of CD4% and Absolute CD4+ T Cell Counts in HIV Infection
Abstract
Introduction: Enumeration of CD4+ T lymphocytes is important for pre-ART disease staging and screening for opportunistic infections, however access to CD4 testing in resource limited settings is poor. Point of care (POC) technologies can facilitate improved access to CD4 testing. We evaluated the analytical performance of a novel POC device the FACSPresto compared to the FACSCalibur as a reference standard and to the PIMA, a POC device in widespread use in sub-Saharan Africa.
Method: Specimens were obtained from 253 HIV infected adults. Venous blood samples were analyzed on the FACSPresto and the FACSCalibur, in a subset of 41 samples additional analysis was done on the PIMA.
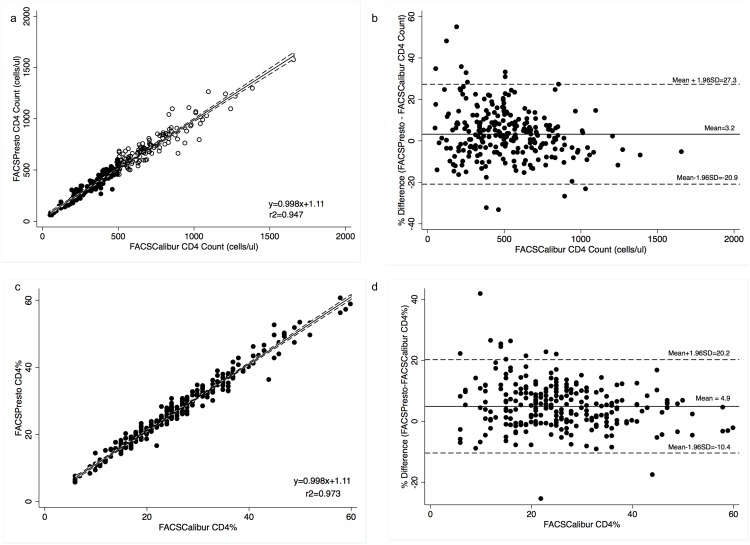
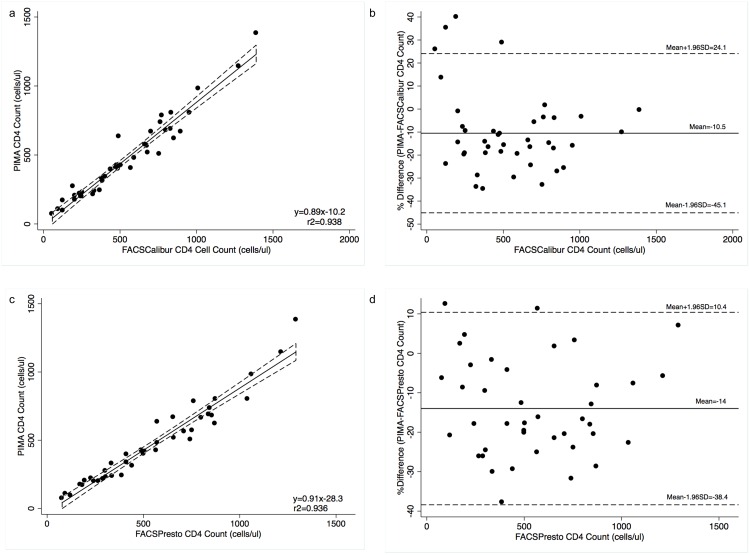
Results: The absolute CD4 count results obtained on the FACSPresto were comparable to those on the FACSCalibur with low absolute (9.5cells/μl) and relative bias (3.2%). Bias in CD4% values was also low (1.06%) with a relative bias of 4.9%. The sensitivity was lower at a CD4 count threshold of ≤350cells/μl compared with ≤500cells/μl (84.9% vs. 92.8%) resulting in a high upward misclassification rate at low CD4 counts. Specificity at thresholds of ≤350cells/μl and ≤500cells/μl were 96.6% and 96.8% respectively. The PIMA had a high absolute (-68.6cells/μl) and relative bias (-10.5%) when compared with the FACSCalibur. At thresholds of ≤350cells/μl and ≤500cells/μl the sensitivity was 100% and 95.5% respectively; specificity was 85.7% and 84.2% respectively. The coefficients of repeatability were 4.13%, 5.29% and 9.8% respectively.
Discussion: The analytic performance of the FACSPresto against the reference standard was very good with better agreement and precision than the PIMA. The FACSPresto had comparable sensitivity at a threshold of 500 cells/μl and better specificity than the PIMA. However the FACSPresto showed reduced sensitivity at low CD4 count thresholds.
Conclusion: The FACSPresto can be reliably used as a POC device for enumerating absolute CD4 count and CD4% values.
Conflict of interest statement
Figures
References
-
- Hogg RS, Yip B, Chan KJ, Wood E, Craib KJ, O'Shaughnessy MV, et al. Rates of disease progression by baseline CD4 cell count and viral load after initiating triple-drug therapy. JAMA. 2001;286(20):2568–77. . - PubMed
-
- Goedert JJ, Biggar RJ, Melbye M, Mann DL, Wilson S, Gail MH, et al. Effect of T4 count and cofactors on the incidence of AIDS in homosexual men infected with human immunodeficiency virus. JAMA. 1987;257(3):331–4. . - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
