

Nonischemic Left Ventricular Scar as a Substrate of Life-Threatening Ventricular Arrhythmias and Sudden Cardiac Death in Competitive Athletes
- PMID: 27390211
- PMCID: PMC4956679
- DOI: 10.1161/CIRCEP.116.004229
Nonischemic Left Ventricular Scar as a Substrate of Life-Threatening Ventricular Arrhythmias and Sudden Cardiac Death in Competitive Athletes
Abstract
Background: The clinical profile and arrhythmic outcome of competitive athletes with isolated nonischemic left ventricular (LV) scar as evidenced by contrast-enhanced cardiac magnetic resonance remain to be elucidated.
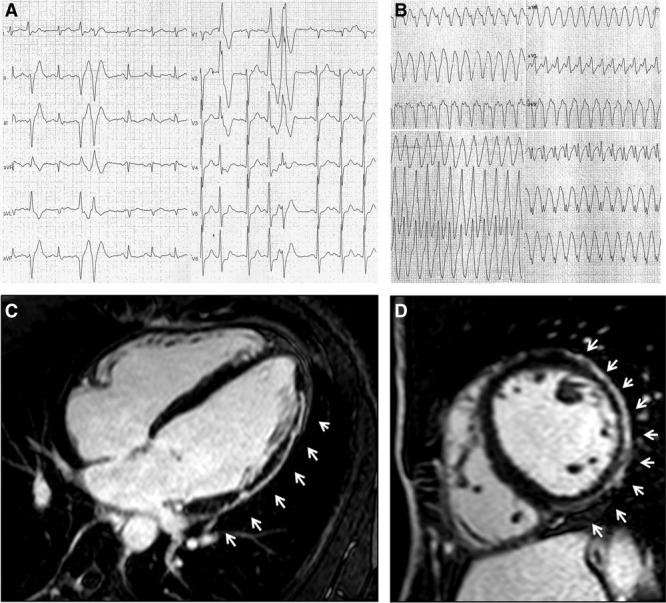
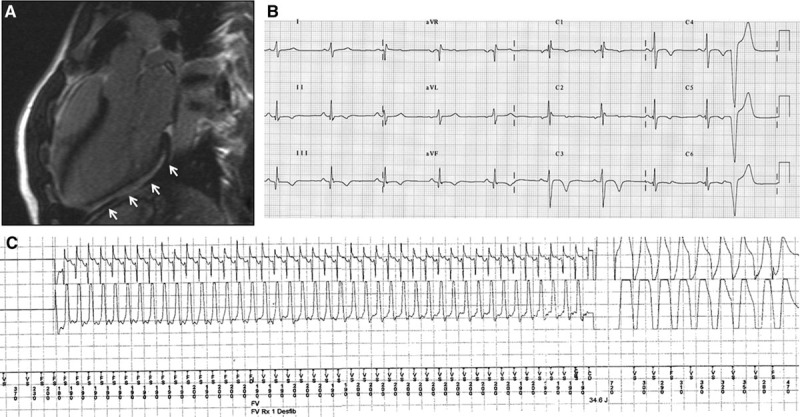
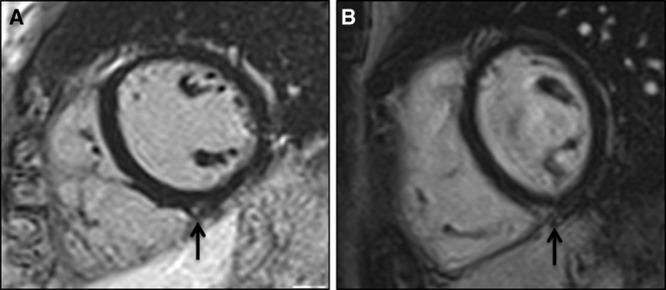
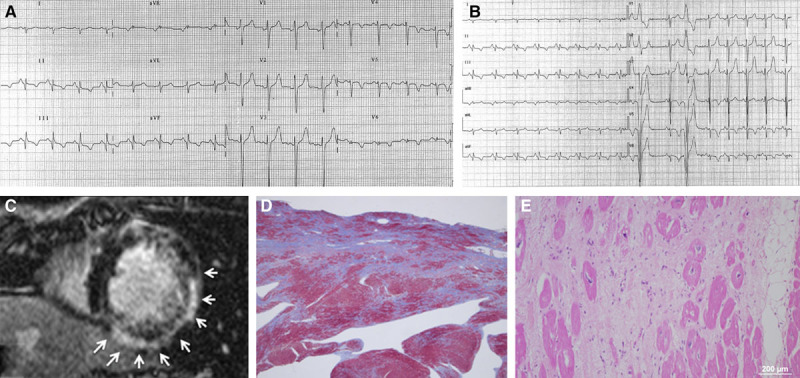
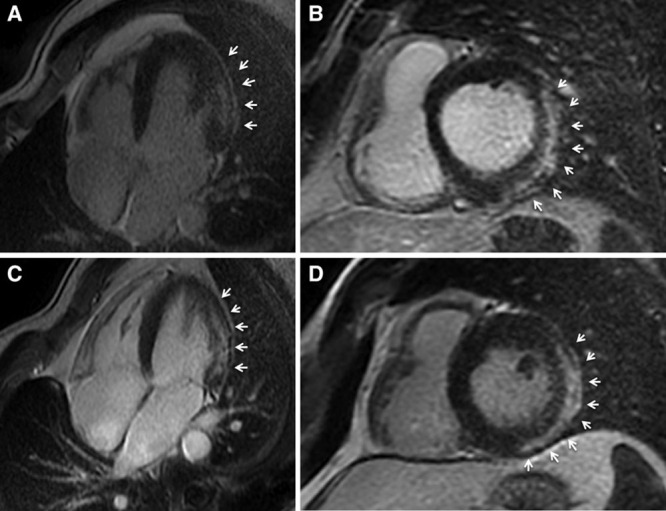
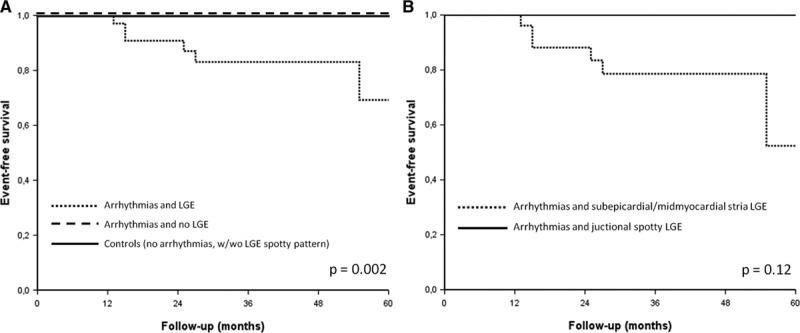
Methods and results: We compared 35 athletes (80% men, age: 14-48 years) with ventricular arrhythmias and isolated LV subepicardial/midmyocardial late gadolinium enhancement (LGE) on contrast-enhanced cardiac magnetic resonance (group A) with 38 athletes with ventricular arrhythmias and no LGE (group B) and 40 healthy control athletes (group C). A stria LGE pattern with subepicardial/midmyocardial distribution, mostly involving the lateral LV wall, was found in 27 (77%) of group A versus 0 controls (group C; P<0.001), whereas a spotty pattern of LGE localized at the junction of the right ventricle to the septum was respectively observed in 11 (31%) versus 10 (25%; P=0.52). All athletes with stria pattern showed ventricular arrhythmias with a predominant right bundle branch block morphology, 13 of 27 (48%) showed ECG repolarization abnormalities, and 5 of 27 (19%) showed echocardiographic hypokinesis of the lateral LV wall. The majority of athletes with no or spotty LGE pattern had ventricular arrhythmias with a predominant left bundle branch block morphology and no ECG or echocardiographic abnormalities. During a follow-up of 38±25 months, 6 of 27 (22%) athletes with stria pattern experienced malignant arrhythmic events such as appropriate implantable cardiac defibrillator shock (n=4), sustained ventricular tachycardia (n=1), or sudden death (n=1), compared with none of athletes with no or LGE spotty pattern and controls.
Conclusions: Isolated nonischemic LV LGE with a stria pattern may be associated with life-threatening arrhythmias and sudden death in the athlete. Because of its subepicardial/midmyocardial location, LV scar is often not detected by echocardiography.
Keywords: athletes; cardiomyopathy; myocarditis; sport; sudden death.
© 2016 The Authors.
Figures
References
-
- Corrado D, Basso C, Rizzoli G, Schiavon M, Thiene G. Does sports activity enhance the risk of sudden death in adolescents and young adults? J Am Coll Cardiol. 2003;42:1959–1963. - PubMed
-
- Corrado D, Basso C, Pavei A, Michieli P, Schiavon M, Thiene G. Trends in sudden cardiovascular death in young competitive athletes after implementation of a preparticipation screening program. JAMA. 2006;296:1593–1601. doi: 10.1001/jama.296.13.1593. - PubMed
-
- Thiene G, Nava A, Corrado D, Rossi L, Pennelli N. Right ventricular cardiomyopathy and sudden death in young people. N Engl J Med. 1988;318:129–133. doi: 10.1056/NEJM198801213180301. - PubMed
-
- Maron BJ. Hypertrophic cardiomyopathy and other causes of sudden cardiac death in young competitive athletes, with considerations for preparticipation screening and criteria for disqualification. Cardiol Clin. 2007;25:399–414, vi. doi: 10.1016/j.ccl.2007.07.006. - PubMed
-
- de Noronha SV, Sharma S, Papadakis M, Desai S, Whyte G, Sheppard MN. Aetiology of sudden cardiac death in athletes in the United Kingdom: a pathological study. Heart. 2009;95:1409–1414. doi: 10.1136/hrt.2009.168369. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
