

Noninvasive Molecular Imaging of Disease Activity in Atherosclerosis
- PMID: 27390335
- PMCID: PMC4939871
- DOI: 10.1161/CIRCRESAHA.116.307971
Noninvasive Molecular Imaging of Disease Activity in Atherosclerosis
Abstract
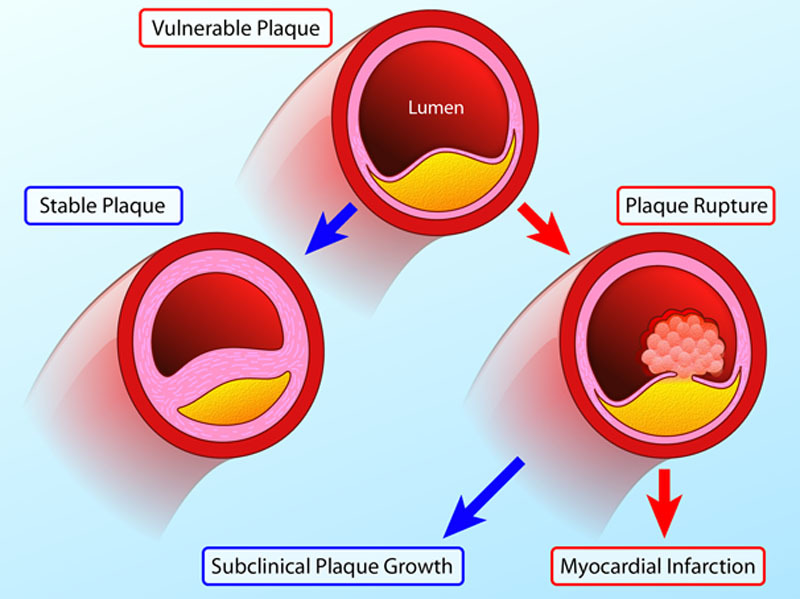
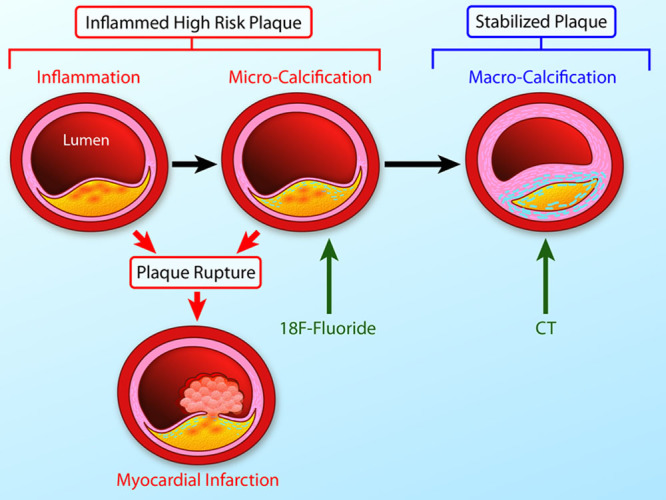
Major focus has been placed on the identification of vulnerable plaques as a means of improving the prediction of myocardial infarction. However, this strategy has recently been questioned on the basis that the majority of these individual coronary lesions do not in fact go on to cause clinical events. Attention is, therefore, shifting to alternative imaging modalities that might provide a more complete pan-coronary assessment of the atherosclerotic disease process. These include markers of disease activity with the potential to discriminate between patients with stable burnt-out disease that is no longer metabolically active and those with active atheroma, faster disease progression, and increased risk of infarction. This review will examine how novel molecular imaging approaches can provide such assessments, focusing on inflammation and microcalcification activity, the importance of these processes to coronary atherosclerosis, and the advantages and challenges posed by these techniques.
Keywords: 18F-Fluorodeoxyglucose; atherosclerosis; disease progression; inflammation; myocardial infarction.
© 2016 The Authors.
Figures
References
-
- Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I. Circulation. 2003;108:1664–1672. doi: 10.1161/01.CIR.0000087480.94275.97. - PubMed
-
- Ambrose JA, Tannenbaum MA, Alexopoulos D, Hjemdahl-Monsen CE, Leavy J, Weiss M, Borrico S, Gorlin R, Fuster V. Angiographic progression of coronary artery disease and the development of myocardial infarction. J Am Coll Cardiol. 1988;12:56–62. - PubMed
-
- Falk E, Shah PK, Fuster V. Coronary plaque disruption. Circulation. 1995;92:657–671. - PubMed
-
- Stone GW, Maehara A, Lansky AJ, de Bruyne B, Cristea E, Mintz GS, Mehran R, McPherson J, Farhat N, Marso SP, Parise H, Templin B, White R, Zhang Z, Serruys PW PROSPECT Investigators. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011;364:226–235. doi: 10.1056/NEJMoa1002358. - PubMed
-
- Calvert PA, Obaid DR, O’Sullivan M, Shapiro LM, McNab D, Densem CG, Schofield PM, Braganza D, Clarke SC, Ray KK, West NE, Bennett MR. Association between IVUS findings and adverse outcomes in patients with coronary artery disease: the VIVA (VH-IVUS in Vulnerable Atherosclerosis) Study. JACC Cardiovasc Imaging. 2011;4:894–901. doi: 10.1016/j.jcmg.2011.05.005. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
