

Differences in nulliparous caesarean section rates across models of care: a decomposition analysis
- PMID: 27392410
- PMCID: PMC4938942
- DOI: 10.1186/s12913-016-1494-3
Differences in nulliparous caesarean section rates across models of care: a decomposition analysis
Abstract
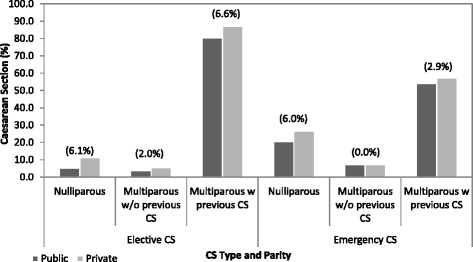
Background: To evaluate the extent of the difference in elective (ELCS) and emergency (EMCS) caesarean section (CS) rates between nulliparous women in public maternity hospitals in Ireland by model of care, and to quantify the contribution of maternal, clinical, and hospital characteristics in explaining the difference in the rates.
Methods: Cross-sectional analysis using a combination of two routinely collected administrative databases was performed. A non-linear extension of the Oaxaca-Blinder method is used to decompose the difference between public and private ELCS and EMCS rates into the proportion explained by the differences in observable maternal, clinical, and hospital characteristics and the proportion that remains unexplained.
Results: Of the 29,870 babies delivered to nulliparous women, 7,792 were delivered via CS (26.1 %), 79.6 % of which were coded as EMCS. Higher prevalence of ELCS was associated with breech presentation, other malpresentation, and the mother being over 40 years old. Higher prevalence of EMCS was associated with placenta praevia or placental abruption, diabetes (pre-existing and gestational), and being over 40 years old. The private model of care is associated with ELCS and EMCS rates 6 percentage points higher compared than the public model of care but this differential is insignificant in the fully adjusted models for EMCS. Just over half (53 %) of the 6 percentage point difference in ELCS rates between the two models of care can be accounted for by maternal, clinical and hospital characteristics. Almost 80 % of the difference for EMCS can be accounted for.
Conclusions: The majority of the difference in EMCS rates across models of care can be explained by differing characteristics between the two groups of women. The main contributor to the difference was advancing maternal age. The unexplained component of the difference for ELCS is larger; an excess private effect remains after accounting for maternal, clinical, and hospital characteristics. This requires further investigation and may be mitigated in future with the introduction of clinical guidelines related to CS.
Keywords: Elective caesarean section; Emergency caesarean section; Non-linear Oaxaca–Blinder decomposition method; Private practice.
Figures
References
-
- Brick A, Layte R: Recent trends in the caesarean section rate in Ireland 1999–2006. ESRI Working Paper 309. 2009. Available at https://www.esri.ie/pubs/WP309.pdf
-
- Brick A, Layte R. Exploring Trends in the Rate of Caesarean Section in Ireland 1999–2007. Econ Soc Rev. 2011;42(4):383–406.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
