

Musculoskeletal manifestations in mucopolysaccharidosis type I (Hurler syndrome) following hematopoietic stem cell transplantation
- PMID: 27392569
- PMCID: PMC4938899
- DOI: 10.1186/s13023-016-0470-7
Musculoskeletal manifestations in mucopolysaccharidosis type I (Hurler syndrome) following hematopoietic stem cell transplantation
Abstract
Background: Hematopoietic stem cell transplantation (HSCT) is the treatment of choice for young Hurler patients. Despite halting of neurocognitive decline and improvement of life expectancy, the beneficial effect on the skeletal system is limited. As orthopedic complications are one of the most disabling factors following HSCT, this points to the need for new treatment strategies. The study summarizes musculoskeletal manifestations in 19 transplanted Hurler patients.
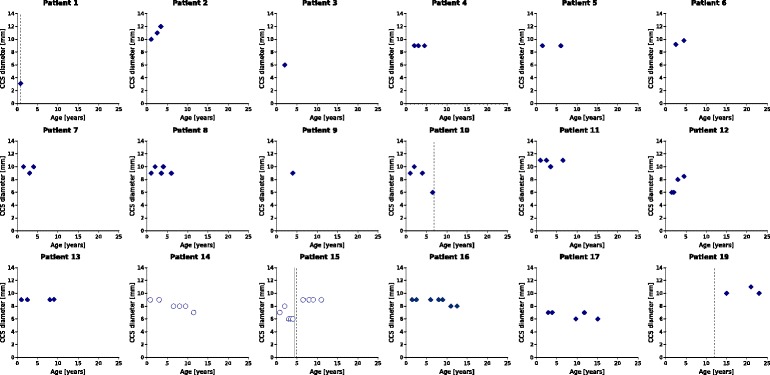
Methods: Data were obtained retrospectively. Patients' charts for physical examinations of the joint range of motion (JROM) of shoulders, elbows, hips and knees were reviewed. Radiographic evaluations of thorax, spine, pelvis and hands were performed. MRI scans of the craniocervical junction were analyzed to determine odontoid hypoplasia and the prevalence of craniocervical stenosis.
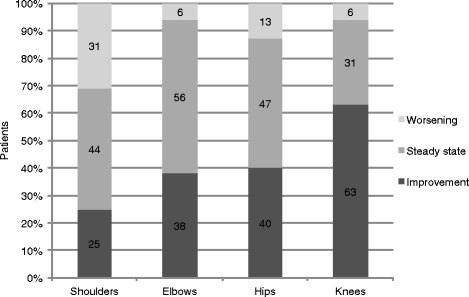
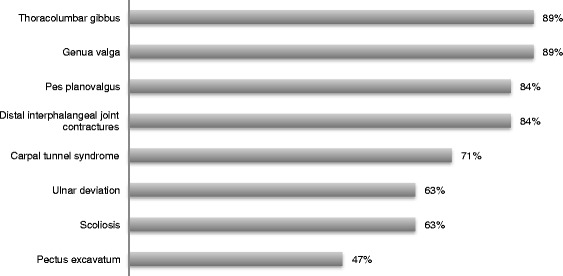
Results: Nineteen Hurler patients (10 females, 9 males) with an average age of 8.1 years (range 2.5-23.8) at the latest follow-up, who underwent allogenic HSCT between 1991 and 2012, were assessed after an average follow-up period of 6.4 years (range 0.7-22.5). Seventeen patients achieved long-term engraftment, two developed graft failures. The majority of patients showed a steady state or improvements in the mobility of knees (31 %/63 %), hips (47 %/40 %) and elbows (56 %/38 %). However, shoulder abduction was impaired in ¾ of patients and showed the highest rate of progression (31 %). In patients with graft failure, progressive restrictions in JROM were noted. Assessments of the craniocervical junction by MRI showed stable or improved diameters in 67 % of patients. Correction or stabilization of odontoid hypoplasia was found in 64 %. However thoracolumbar kyphosis, scoliosis, hip dysplasia and genua valga were progressive despite HSCT. At the last follow up, 47 % of patients were partially wheelchair dependent, 10 % wheelchair bound and 25 % regularly experienced pain in the spine, hips and lower extremities due to orthopedic problems.
Conclusion: Joint mobility, odontoid hypoplasia and craniocervical stenosis might stabilize or even improve in Hurler patients following HSCT. However, despite the beneficial effects on some musculoskeletal manifestations, skeletal complications are frequently observed and the overall burden of orthopedic disease is significant. Frequent multi-disciplinary follow-up in a specialized center are essential. Novel therapeutic approaches (e.g. anti-inflammatory drugs) are needed to improve musculoskeletal outcomes.
Keywords: Craniocervical stenosis; Dysostosis multiplex; Hip dysplasia; Hurler syndrome; Mucopolysaccharidosis type I; Musculoskeletal manifestations; Odontoid hypoplasia; Thoracolumbar kyphosis.
Figures
References
-
- Neufeld EF, Muenzer J. The mucopolysaccharidoses. In: Scriver CR, Beaudet AL, Sly WS, Valle D, editors. The metabolic & molecular bases of inherited disease. 8. New York: McGraw-Hill; 2001. pp. 3421–52.
-
- De R, Minke H, Teunissen QG, der Lee V, Johanna H, Beck M, Bodamer OA, Clarke LA, Hollak CE, Lin S, Rojas MM, Pastores GM, Raiman JA, Scarpa M, Treacy EP, Tylki-Szymanska A, Wraith JE, Zeman J, Wijburg FA. Capturing phenotypic heterogeneity in MPS I: results of an international consensus procedure. Orphanet J Rare Dis. 2012;7:22. doi: 10.1186/1750-1172-7-22. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
