

Diagnostic methods in ocular argyrosis: case report
- PMID: 27392933
- PMCID: PMC5052328
- DOI: 10.1007/s10633-016-9552-z
Diagnostic methods in ocular argyrosis: case report
Abstract
Purpose: The aim of this report is to present a case of a patient, metal foundry worker, who had been exposed to industrial silver salts for over 20 years. It is well established that chronic exposure to silver compounds can cause accumulation of silver deposits in various tissues. This condition is referred to as argyrosis or argyria, whereas changes related to eye tissues are defined as ocular argyrosis.
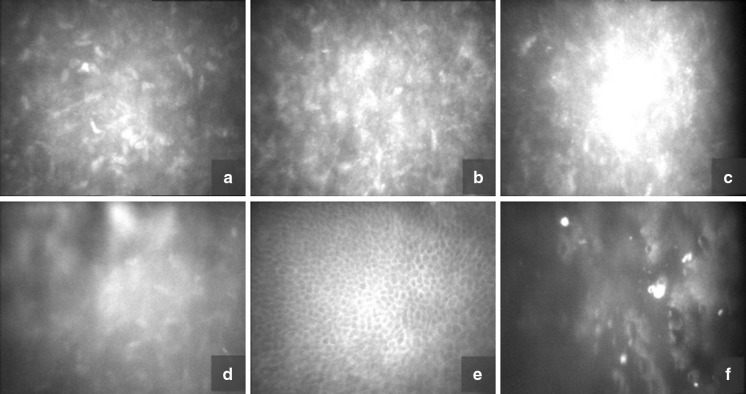
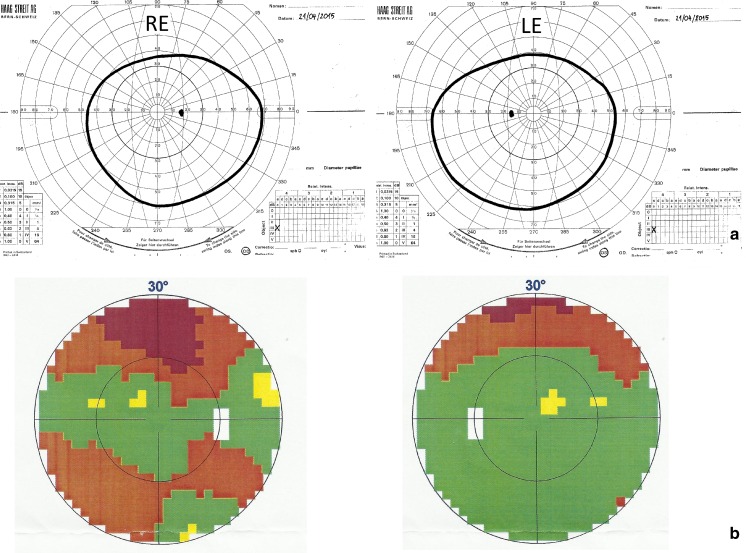
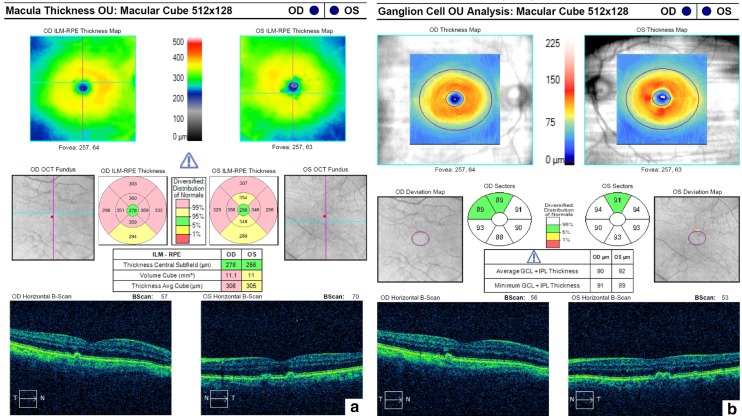
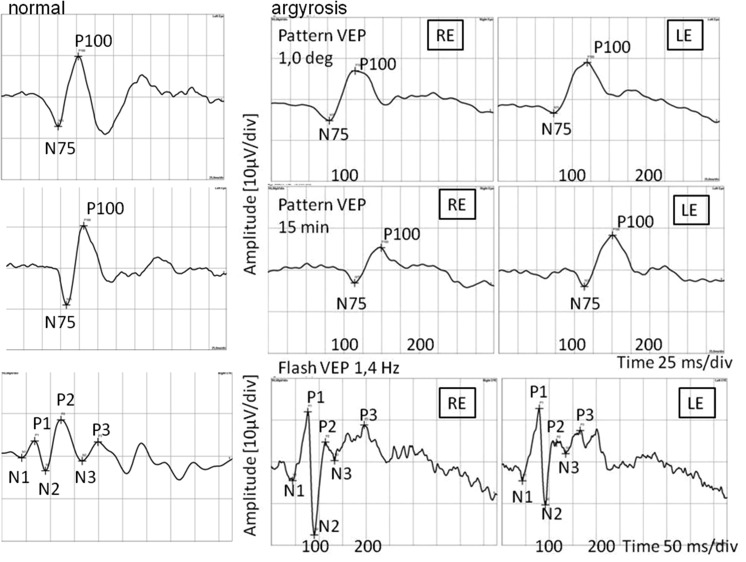
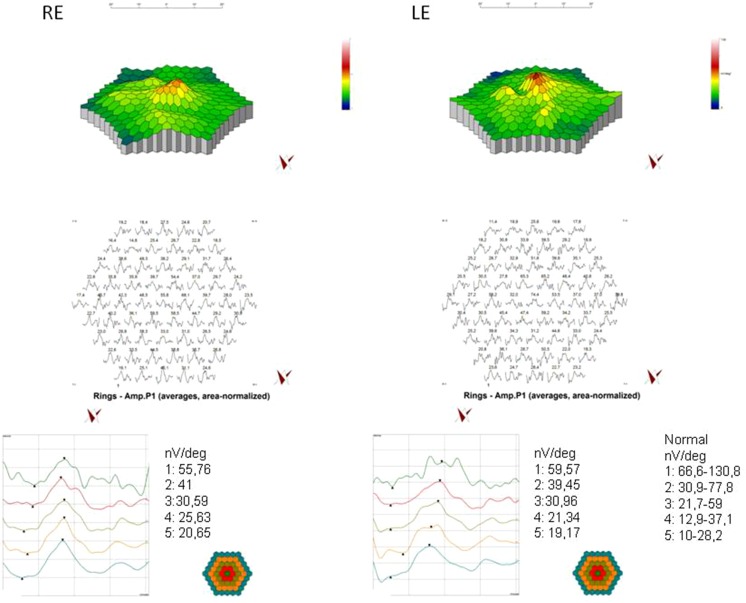
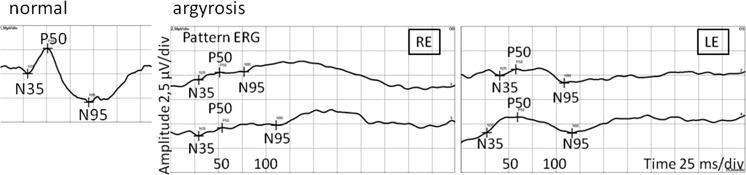
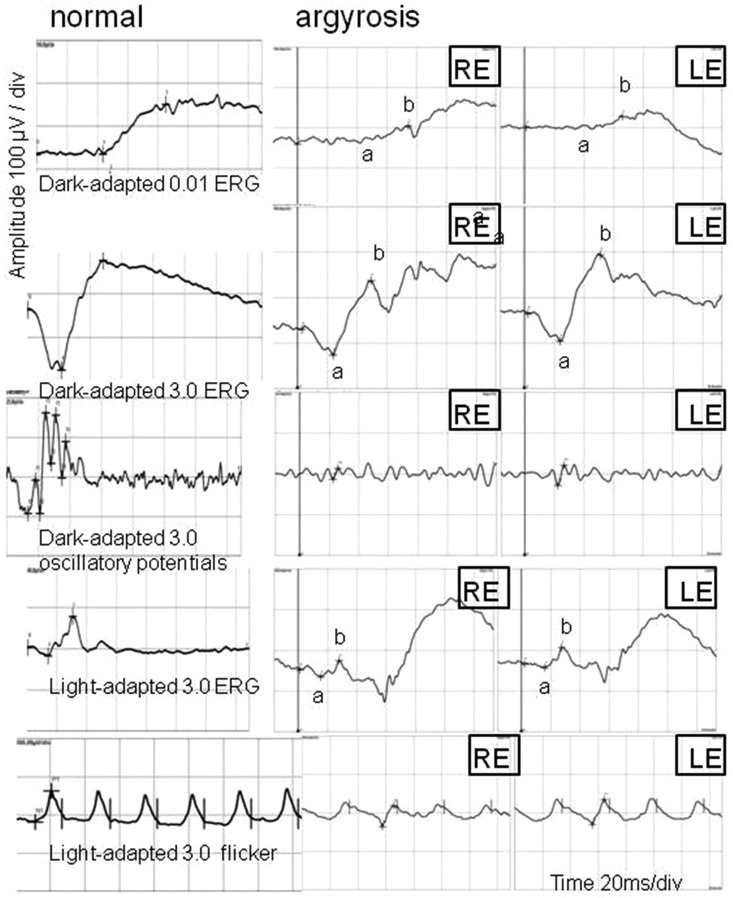
Methods: A complete eye examination, corneal confocal microscopy, kinetic and static visual field test, posterior segment optical coherent tomography, pattern visual evoked potentials (PVEP), flash visual evoked potentials, multifocal electroretinogram, pattern electroretinogram (PERG), full-field electroretinography (FERG) and electrooculogram were all performed.
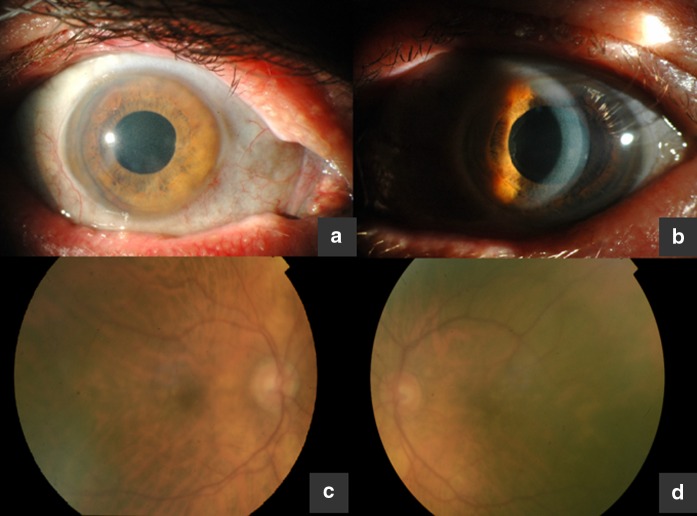
Results: Eye examination revealed decreased visual acuity, corneal deposits and drusenoid changes within the macula. Although electrophysiology tests did not show changes in the function of retinal pigment epithelium, they revealed abnormal function of photoreceptors in the central and peripheral retina. PERG abnormalities and delayed latency of P100 wave in PVEP confirmed impaired function of the inner layers of the retina in the macular region.
Conclusions: Corneal confocal microscopy and electrophysiological tests may help confirm the diagnosis of ocular argyrosis.
Keywords: Argyria; Argyrosis; Ocular argyrosis; Silver nitrate.
Conflict of interest statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interests; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript. Ethical approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study was approved by the Ethics Committee of Medical University of Silesia, Katowice, Poland. Informed consent Informed consent was obtained from all individual participants included in the study. Statement of human rights and statement on the welfare of animals The study protocol was adhered to the tenets of the Declaration of Helsinki. 10.1007/s10633-016-9552-z
Figures
References
-
- Wadhera A, Fung M. Systemic argyria associated with ingestion of colloidal silver. Dermatol Online J. 2005;11(1):12. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
