

Influence of timing, radiation, and reconstruction on complications and speech outcomes with tracheoesophageal puncture
- PMID: 27394060
- PMCID: PMC5118069
- DOI: 10.1002/hed.24529
Influence of timing, radiation, and reconstruction on complications and speech outcomes with tracheoesophageal puncture
Abstract
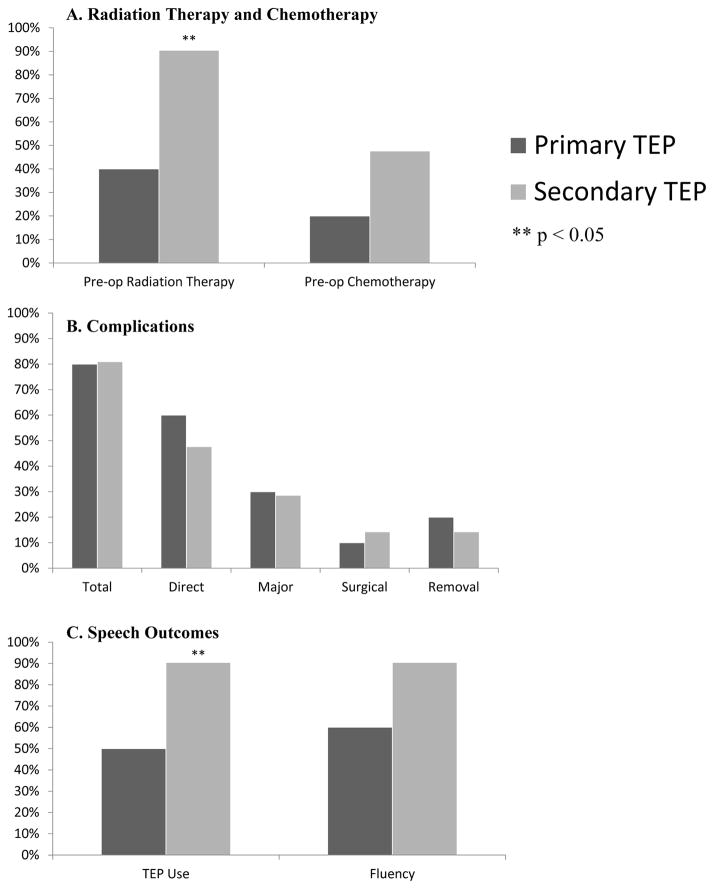
Background: We evaluated the impact of radiation, reconstruction, and timing of tracheoesophageal puncture (TEP) on complications and speech outcomes.
Methods: Retrospective review identified 145 patients who underwent TEP between 2003 and 2007.
Results: Ninety-nine patients (68%) had primary and 46 (32%) had secondary TEP, with complications occurring in 65% and 61%, respectively (p = .96). Twenty-nine patients (20%) had major complications (18 primary and 11 secondary; p = .42). Ninety-four patients (65%) had pre-TEP radiation, 39 (27%) post-TEP radiation, and 12 (8%) no radiation. With patients grouped by TEP timing and radiation history, there was no difference in complications, fluency, or TEP use. With mean 4.7-year follow-up, 82% primary and 85% secondary used TEP for primary communication (p = .66). Free-flap patients used TEP more commonly for primary communication after secondary versus primary TEP (90% vs 50%; p = .02).
Conclusion: Primary and secondary tracheoesophageal speakers experience similar high rates of complications. Extent of pharyngeal reconstruction, rather than radiation, may be more important in selection of TEP timing. © 2016 Wiley Periodicals, Inc. Head Neck 38: 1765-1771, 2016.
Keywords: complications; speech outcomes; tracheoesophageal prosthesis; tracheoesophageal puncture (TEP).
© 2016 Wiley Periodicals, Inc.
Figures

References
-
- Robertson SM, Yeo JC, Dunnet C, Young D, Mackenzie K. Voice, swallowing, and quality of life after total laryngectomy: results of the west of Scotland laryngectomy audit. Head Neck. 2012;34:59–65. - PubMed
-
- Stafford FW. Current indications and complications of tracheoesophageal puncture for voice restoration after laryngectomy. Curr Opin Otolaryngol Head Neck Surg. 2003;11:89–95. - PubMed
-
- Singer MI, Blom ED. An endoscopic technique for restoration of voice after laryngectomy. Ann Otol Rhinol Laryngol. 1980;89:529–33. - PubMed
-
- Cheng E, Ho M, Ganz C, et al. Outcomes of primary and secondary tracheoesophageal puncture: a 16-year retrospective analysis. Ear Nose Throat J. 2006;85:264–7. - PubMed
-
- Op de Coul BM, Hilgers F, Balm AJ, et al. A decade of post laryngectomy vocal rehabilitation in 318 patients. Arch Otolaryngol Head Neck Surg. 2000;126:1320–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
