

Characterization of erythropoietin and hepcidin in the regulation of persistent injury-associated anemia
- PMID: 27398985
- PMCID: PMC5028270
- DOI: 10.1097/TA.0000000000001163
Characterization of erythropoietin and hepcidin in the regulation of persistent injury-associated anemia
Abstract
Background: The cause of persistent injury-associated anemia is multifactorial and includes acute blood loss, an altered erythropoietin (EPO) response, dysregulation of iron homeostasis, and impaired erythropoiesis in the setting of chronic inflammation/stress. Hepcidin plays a key role in iron homeostasis and is regulated by anemia and inflammation. Erythropoietin is a main regulator of erythropoiesis induced by hypoxia. A unique rodent model of combined lung injury (LC)/hemorrhagic shock (HS) (LCHS)/chronic restraint stress (CS) was used to produce persistent injury-associated anemia to further investigate the roles of EPO, hepcidin, iron, ferritin, and the expression of EPO receptors (EPOr).
Methods: Male Sprague-Dawley rats were randomly assigned into one of the four groups of rodent models: naive, CS alone, combined LCHS, or LCHS/CS. Plasma was used to evaluate levels of EPO, hepcidin, iron, and ferritin. RNA was isolated from bone marrow and lung tissue to evaluate expression of EPOr. Comparisons between models were performed by t tests followed by one-way analysis of variance.
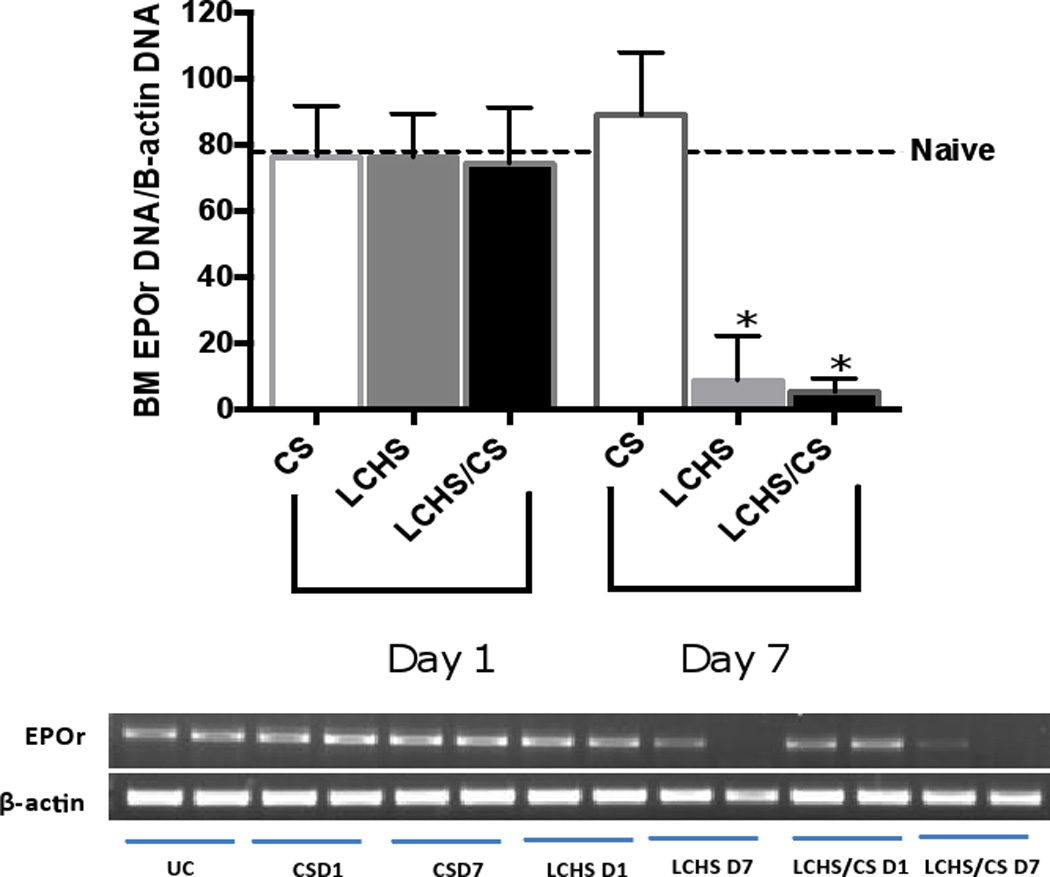
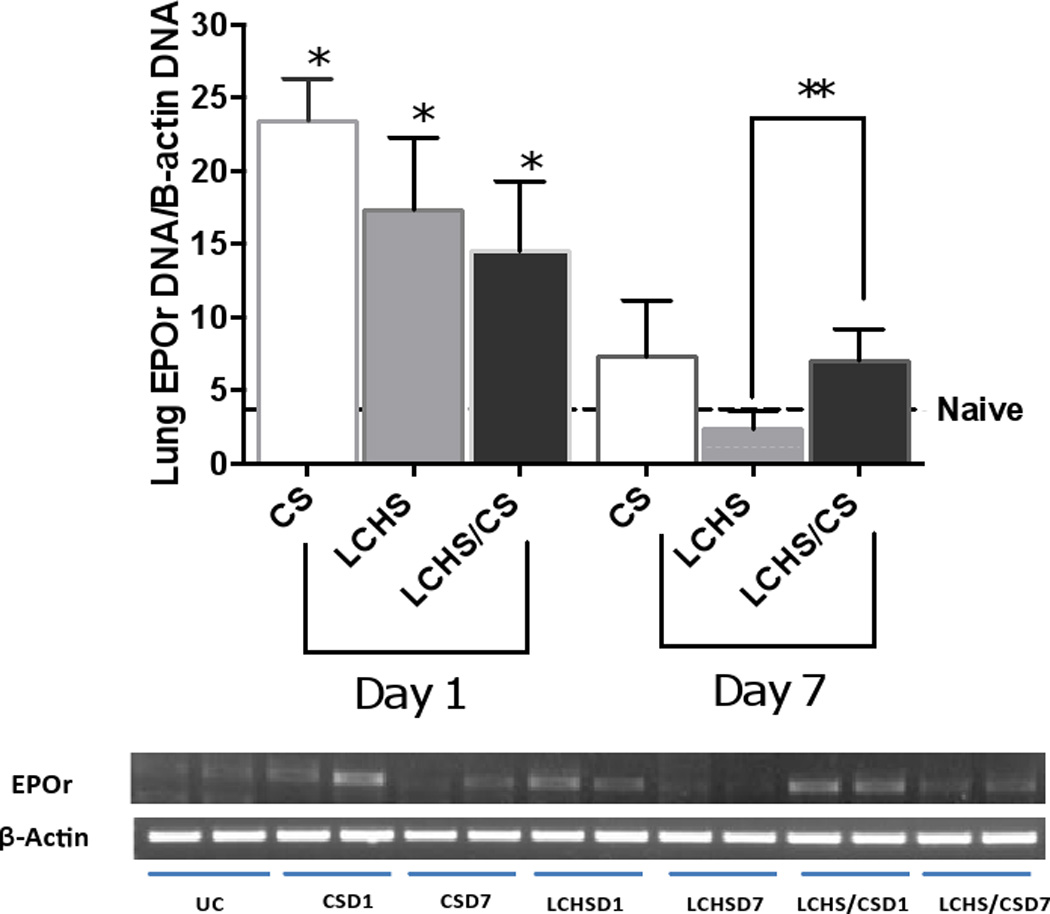
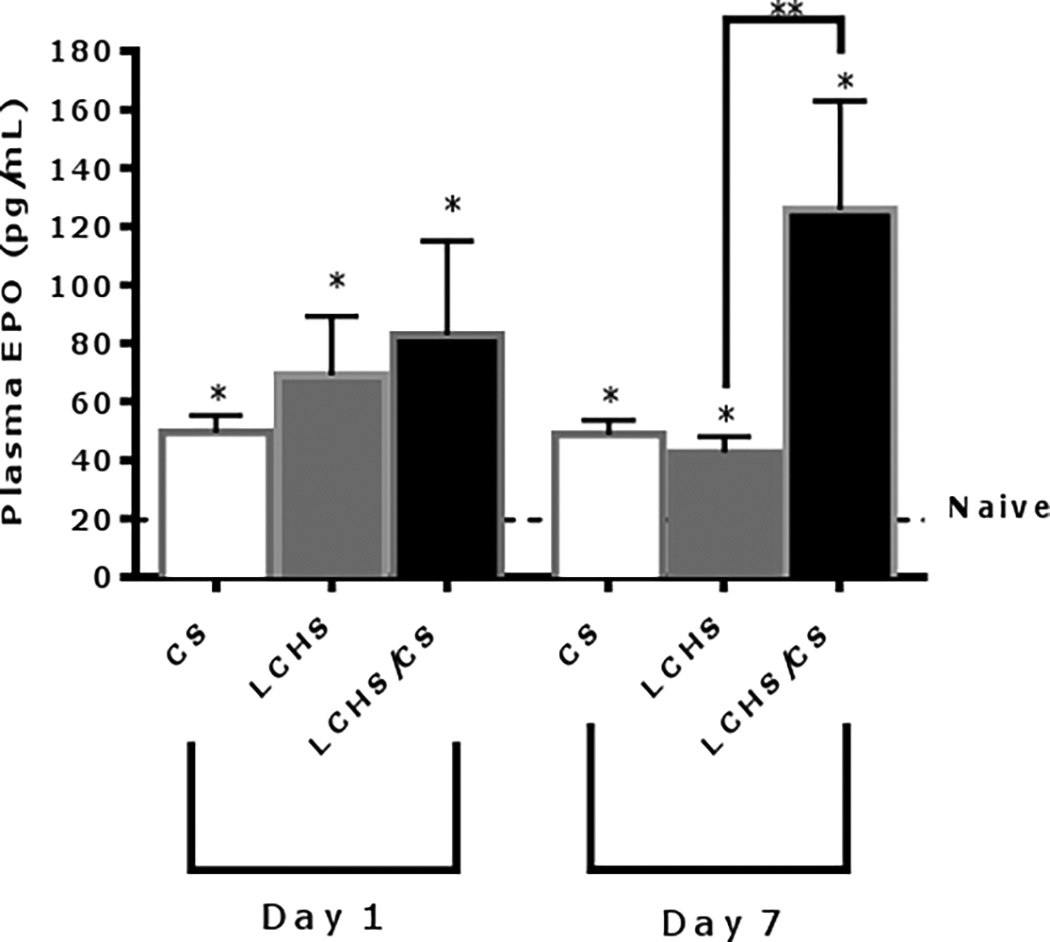
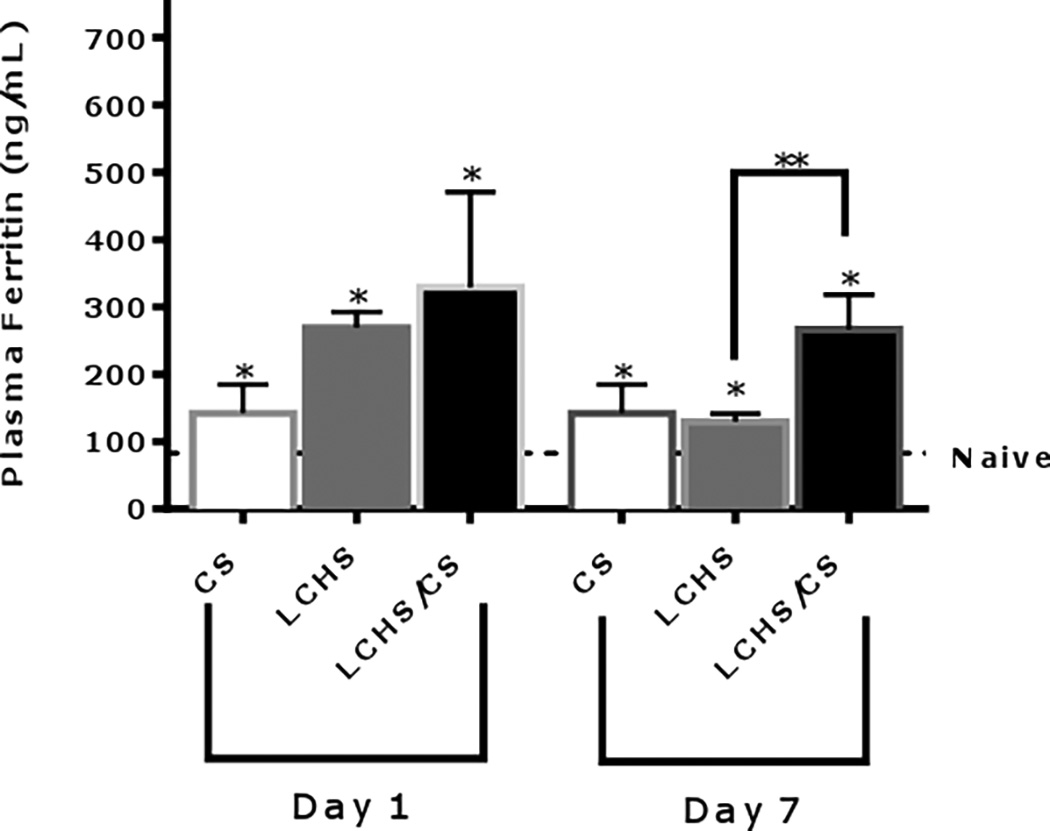
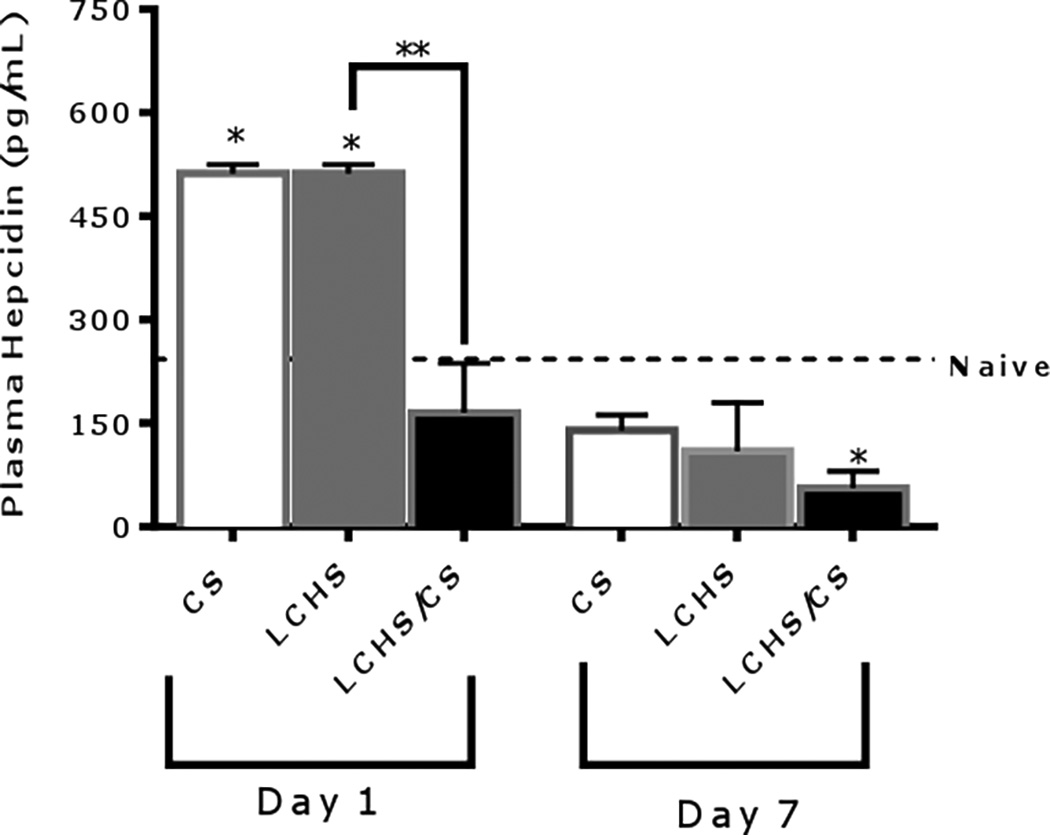
Results: After 7 days, only LCHS/CS was associated with persistent anemia despite significant elevation of plasma EPO. Combined LCHS and LCHS/CS led to a persistent decrease in EPOr expression in bone marrow on Day 7. The LCHS/CS significantly decreased plasma hepcidin levels by 75% on Day 1 and 84% on Day 7 compared to LCHS alone. Hepcidin plasma levels are inversely proportional to EPO plasma levels (Pearson R = -0.362, p < 0.05).
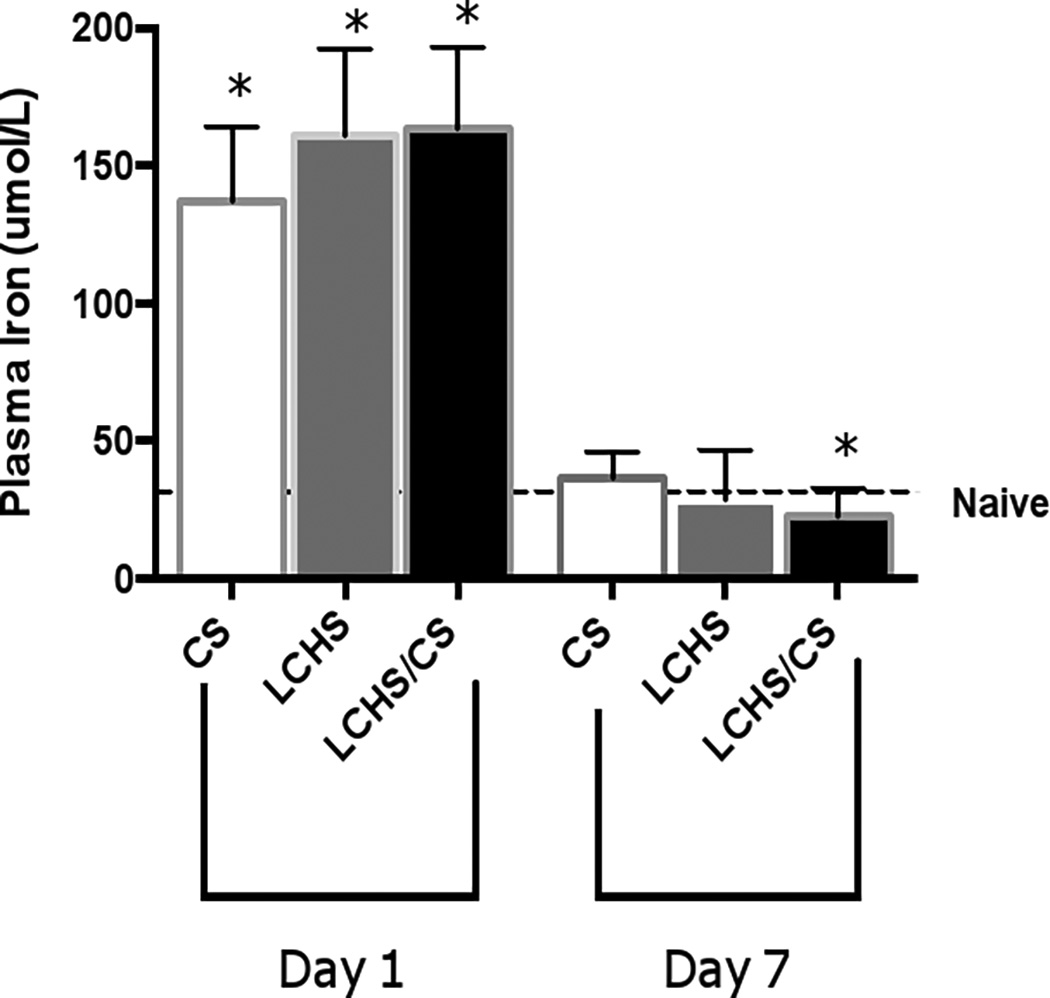
Conclusion: Tissue injury, hemorrhagic shock, and stress stimulate and maintain high levels of plasma EPO while hepcidin levels are decreased. In addition, bone marrow EPOr and plasma iron availability are significantly reduced following LCHS/CS. The combined deficit of reduced iron availability and reduced bone marrow EPOr expression may play a key role in the ineffective EPO response associated with persistent injury-associated anemia.
Figures
References
-
- Corwin HL, Gettinger A, Pearl RG, Fink MP, Levy MM, Abraham E, MacIntyre NR, Shabot MM, Duh MS, Shapiro MJ. The CRIT Study: Anemia and blood transfusion in the critically ill--current clinical practice in the United States. Crit Care Med. 2004;32(1):39–52. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
