

Sexual Dimorphism in Adverse Pregnancy Outcomes - A Retrospective Australian Population Study 1981-2011
- PMID: 27398996
- PMCID: PMC4939964
- DOI: 10.1371/journal.pone.0158807
Sexual Dimorphism in Adverse Pregnancy Outcomes - A Retrospective Australian Population Study 1981-2011
Abstract
Objectives: Sexual inequality starts in utero. The contribution of biological sex to the developmental origins of health and disease is increasingly recognized. The aim of this study was to assess and interpret sexual dimorphisms for three major adverse pregnancy outcomes which affect the health of the neonate, child and potentially adult.
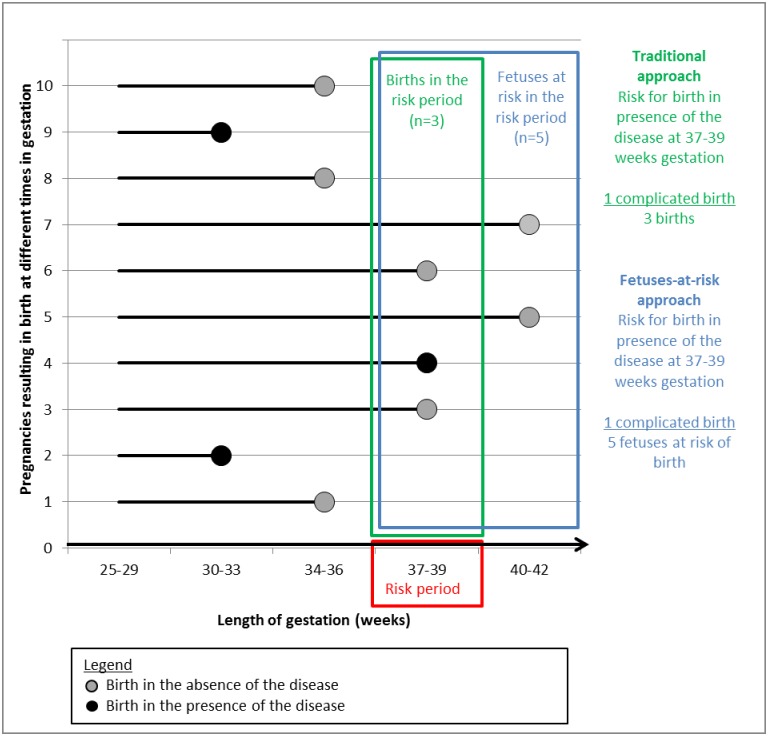
Methods: Retrospective population-based study of 574,358 South Australian singleton live births during 1981-2011. The incidence of three major adverse pregnancy outcomes [preterm birth (PTB), pregnancy induced hypertensive disorders (PIHD) and gestational diabetes mellitus (GDM)] in relation to fetal sex was compared according to traditional and fetus-at-risk (FAR) approaches.
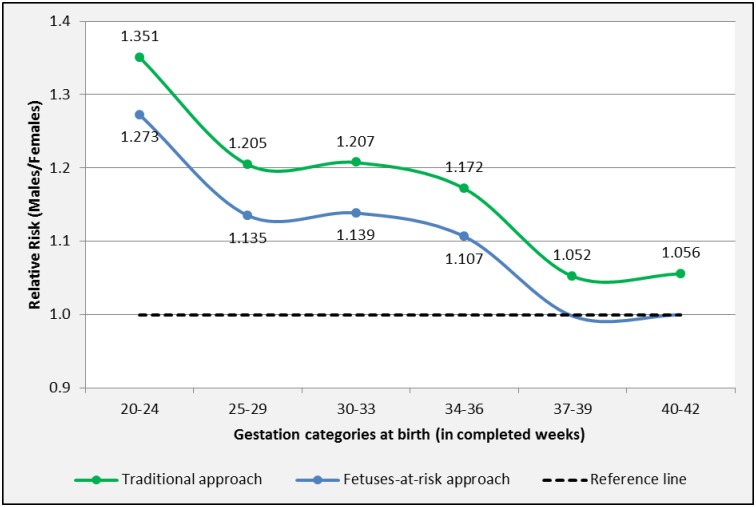
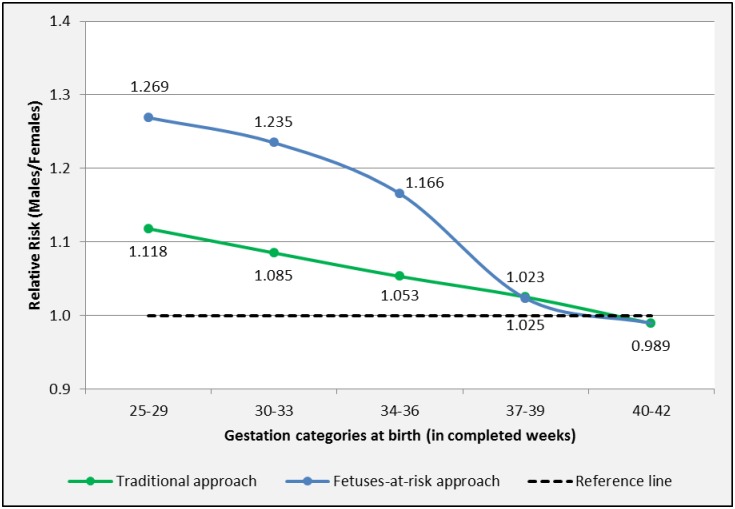
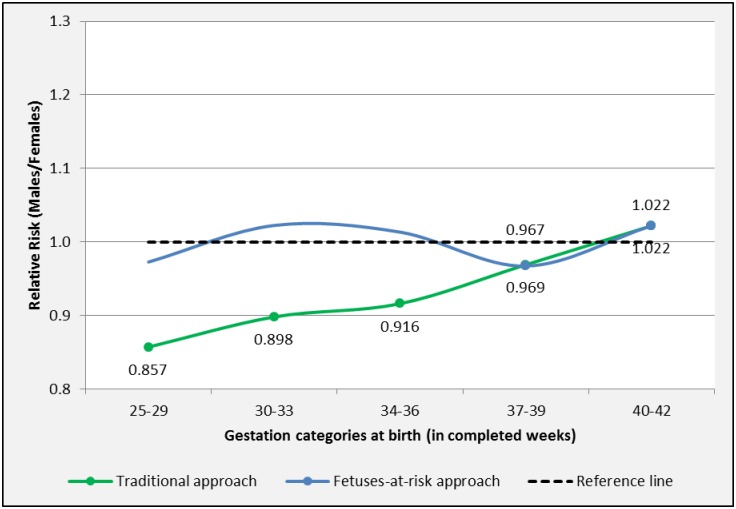
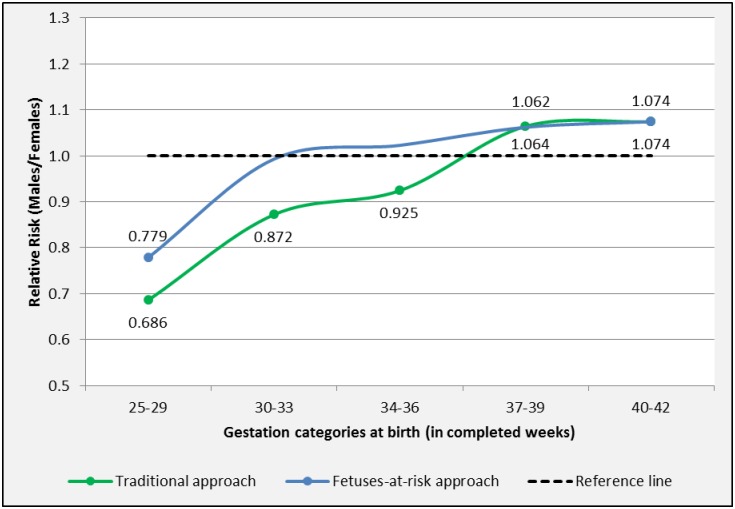
Results: The traditional approach showed male predominance for PTB [20-24 weeks: Relative Risk (RR) M/F 1.351, 95%-CI 1.274-1.445], spontaneous PTB [25-29 weeks: RR M/F 1.118, 95%-CI 1.044-1.197%], GDM [RR M/F 1.042, 95%-CI 1.011-1.074], overall PIHD [RR M/F 1.053, 95%-CI 1.034-1.072] and PIHD with term birth [RR M/F 1.074, 95%-CI 1.044-1.105]. The FAR approach showed that males were at increased risk for PTB [20-24 weeks: RR M/F 1.273, 95%-CI 1.087-1.490], for spontaneous PTB [25-29 weeks: RR M/F 1.269, 95%-CI 1.143-1.410] and PIHD with term birth [RR M/F 1.074, 95%-CI 1.044-1.105%]. The traditional approach demonstrated female predominance for iatrogenic PTB [25-29 weeks: RR M/F 0.857, 95%-CI 0.780-0.941] and PIHD associated with PTB [25-29 weeks: RR M/F 0.686, 95%-CI 0.581-0.811]. The FAR approach showed that females were at increased risk for PIHD with PTB [25-29 weeks: RR M/F 0.779, 95%-CI 0.648-0.937].
Conclusions: This study confirms the presence of sexual dimorphisms and presents a coherent framework based on two analytical approaches to assess and interpret the sexual dimorphisms for major adverse pregnancy outcomes. The mechanisms by which these occur remain elusive, but sex differences in placental gene expression and function are likely to play a key role. Further research on sex differences in placental function and maternal adaptation to pregnancy is required to delineate the causal molecular mechanisms in sex-specific pregnancy outcome. Identifying these mechanisms may inform fetal sex specific tailored antenatal and neonatal care.
Conflict of interest statement
Figures
References
-
- Tranquilli AL, Landi B, Giannubilo SR, Sibai BM. Preeclampsia: No longer solely a pregnancy disease. Pregnancy Hypertens An Int J Women’s Cardiovasc Heal. International Society for the Study of Hypertension in Pregnancy; 2012;2(4):350–7. - PubMed
-
- Di Renzo G, Rosati A, Sarti R, Cruciani L, Cutuli A. Does fetal sex affect pregnancy outcome? Gend Med. 2007;4(1):19–30. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
