

Empirical Evidence of Study Design Biases in Randomized Trials: Systematic Review of Meta-Epidemiological Studies
- PMID: 27398997
- PMCID: PMC4939945
- DOI: 10.1371/journal.pone.0159267
Empirical Evidence of Study Design Biases in Randomized Trials: Systematic Review of Meta-Epidemiological Studies
Abstract
Objective: To synthesise evidence on the average bias and heterogeneity associated with reported methodological features of randomized trials.
Design: Systematic review of meta-epidemiological studies.
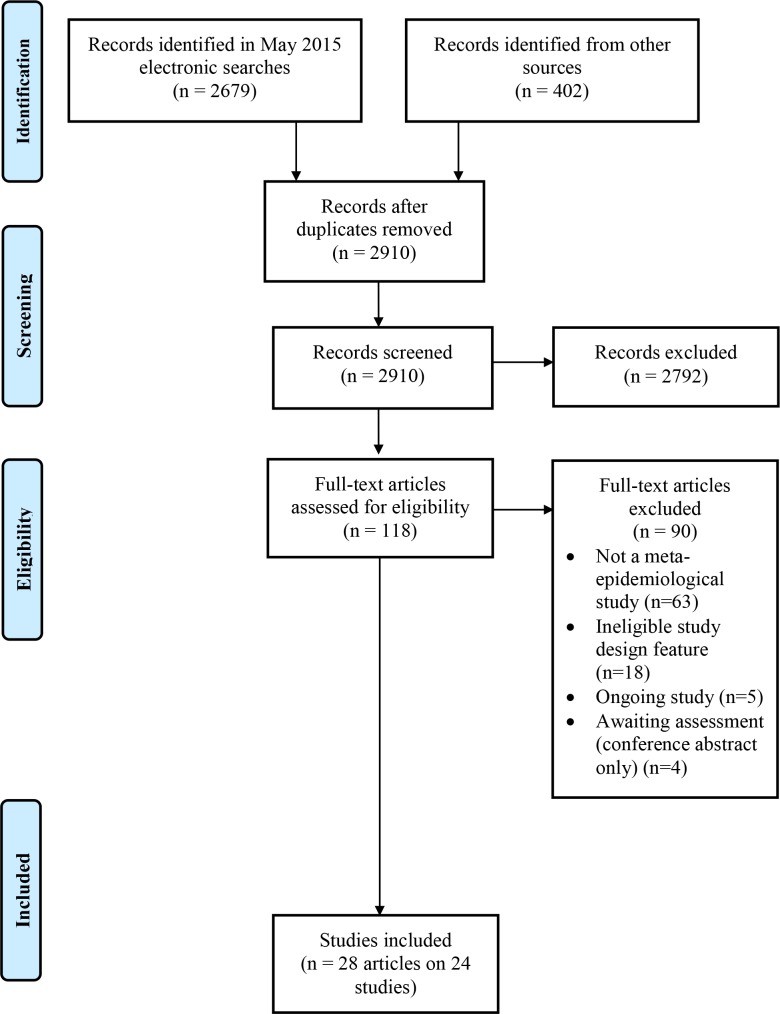
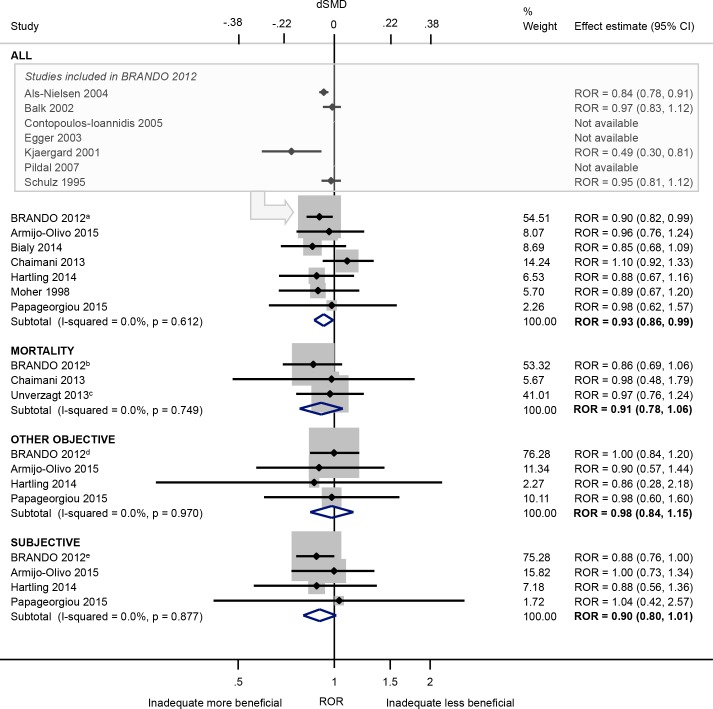
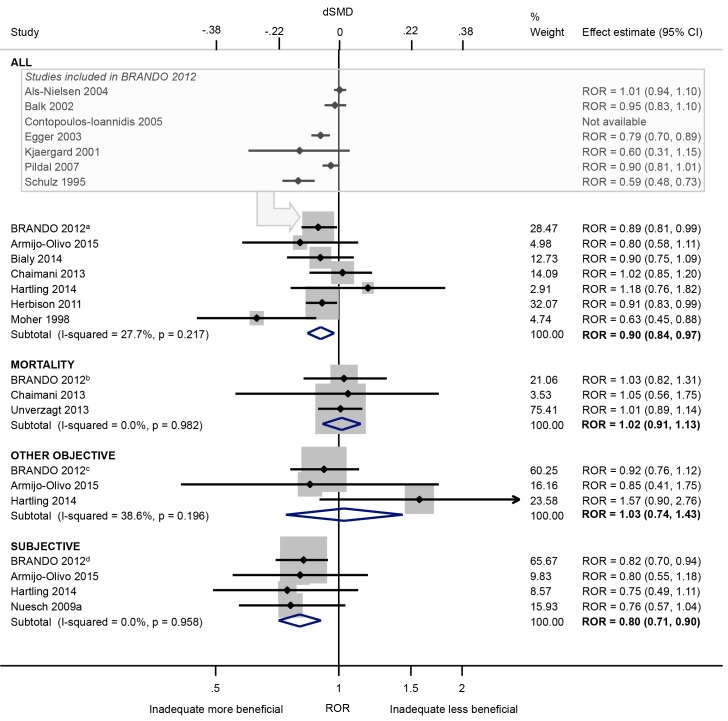
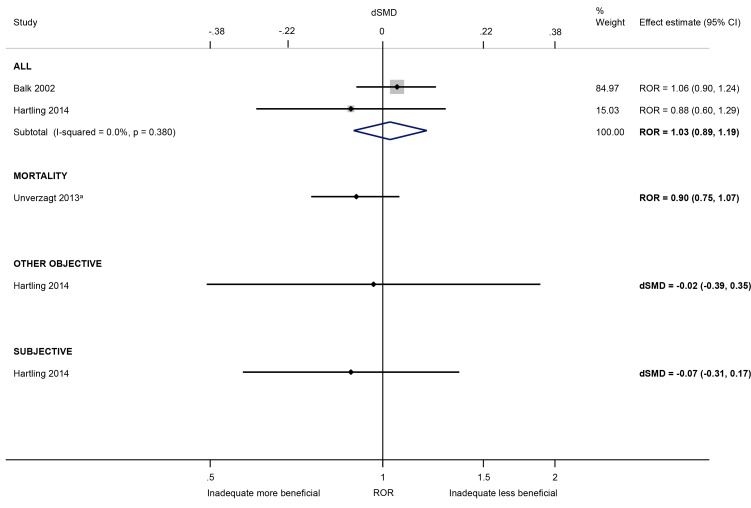
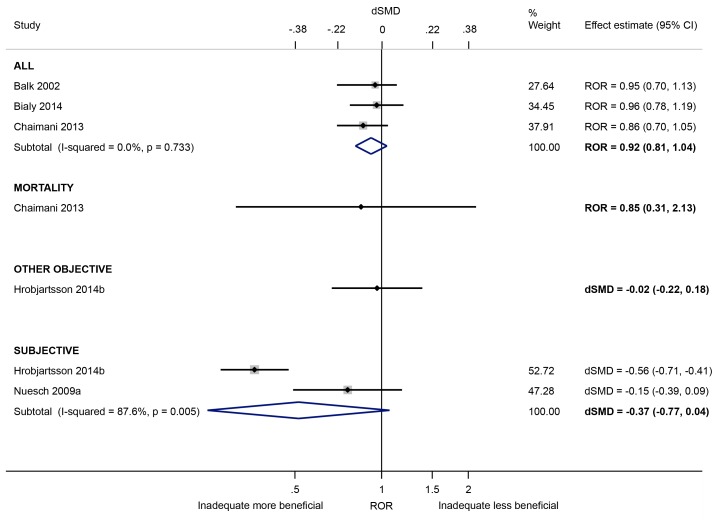
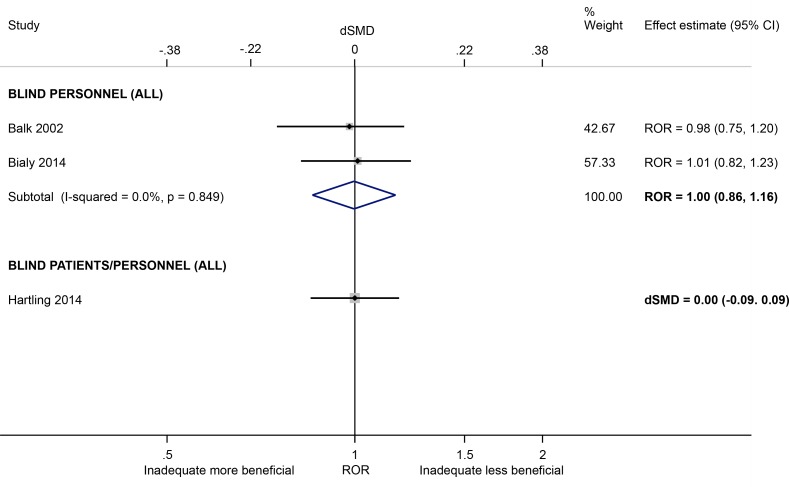
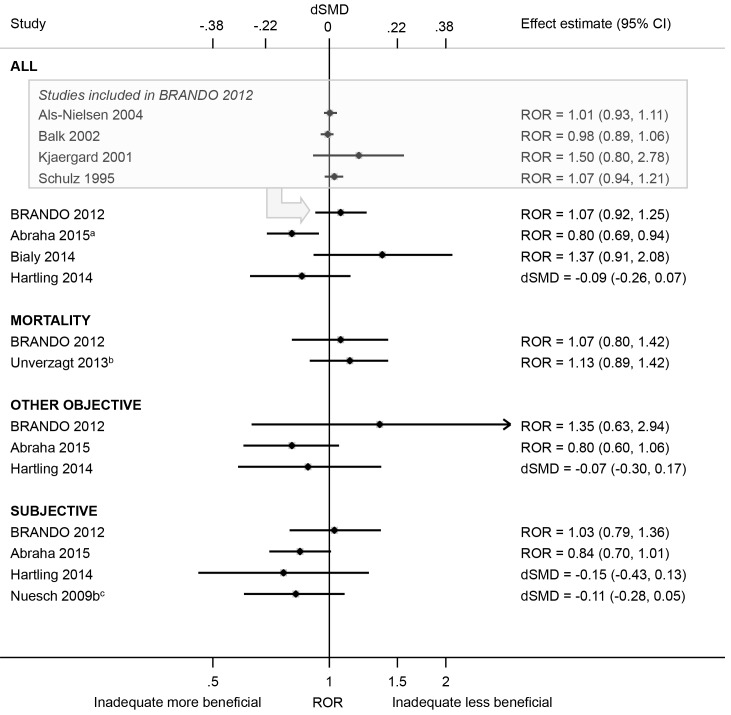
Methods: We retrieved eligible studies included in a recent AHRQ-EPC review on this topic (latest search September 2012), and searched Ovid MEDLINE and Ovid EMBASE for studies indexed from Jan 2012-May 2015. Data were extracted by one author and verified by another. We combined estimates of average bias (e.g. ratio of odds ratios (ROR) or difference in standardised mean differences (dSMD)) in meta-analyses using the random-effects model. Analyses were stratified by type of outcome ("mortality" versus "other objective" versus "subjective"). Direction of effect was standardised so that ROR < 1 and dSMD < 0 denotes a larger intervention effect estimate in trials with an inadequate or unclear (versus adequate) characteristic.
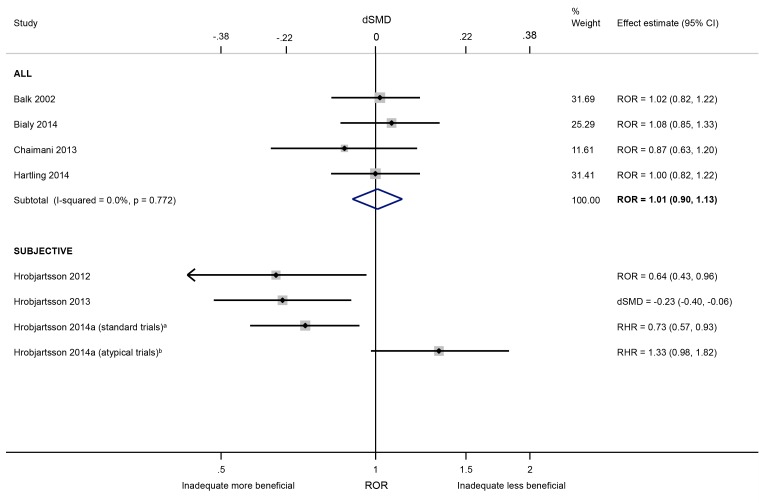
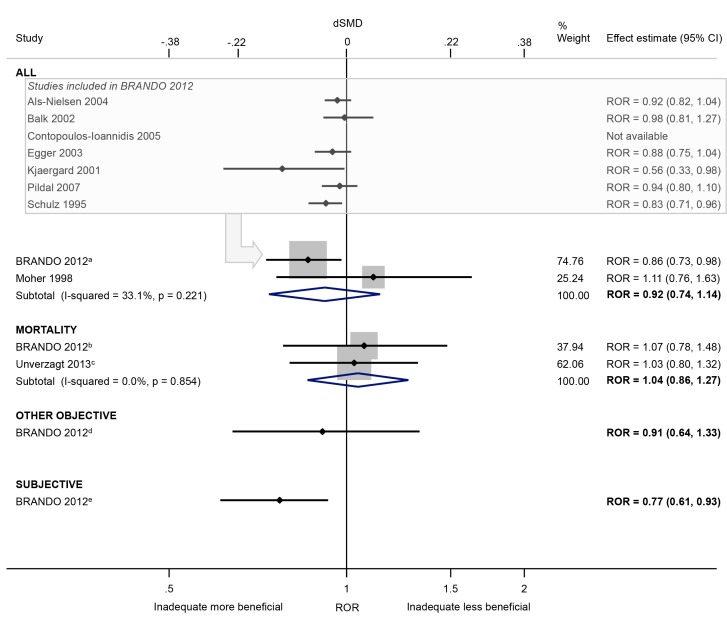
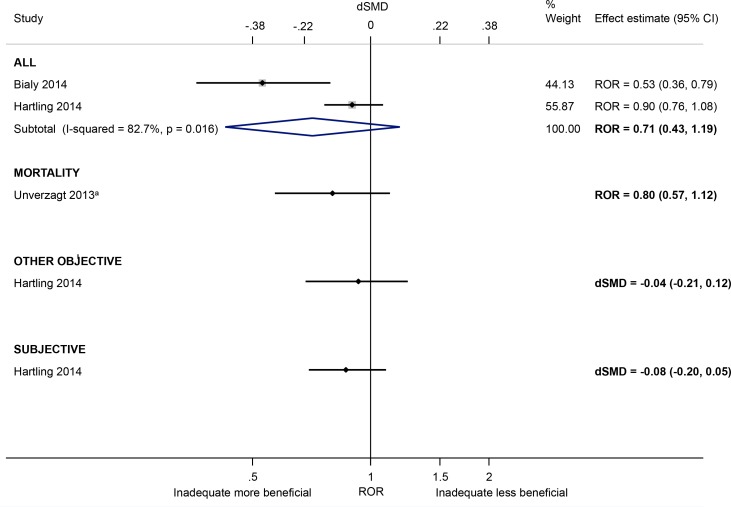
Results: We included 24 studies. The available evidence suggests that intervention effect estimates may be exaggerated in trials with inadequate/unclear (versus adequate) sequence generation (ROR 0.93, 95% CI 0.86 to 0.99; 7 studies) and allocation concealment (ROR 0.90, 95% CI 0.84 to 0.97; 7 studies). For these characteristics, the average bias appeared to be larger in trials of subjective outcomes compared with other objective outcomes. Also, intervention effects for subjective outcomes appear to be exaggerated in trials with lack of/unclear blinding of participants (versus blinding) (dSMD -0.37, 95% CI -0.77 to 0.04; 2 studies), lack of/unclear blinding of outcome assessors (ROR 0.64, 95% CI 0.43 to 0.96; 1 study) and lack of/unclear double blinding (ROR 0.77, 95% CI 0.61 to 0.93; 1 study). The influence of other characteristics (e.g. unblinded trial personnel, attrition) is unclear.
Conclusions: Certain characteristics of randomized trials may exaggerate intervention effect estimates. The average bias appears to be greatest in trials of subjective outcomes. More research on several characteristics, particularly attrition and selective reporting, is needed.
Conflict of interest statement
Figures
References
-
- Guyatt G, Cairns J, Churchill D, Cook D, Haynes B, Hirsh J, et al. Evidence-based medicine: A new approach to teaching the practice of medicine. JAMA. 1992;268(17):2420–5. - PubMed
-
- NHMRC. How to use the evidence: assessment and application of scientific evidence Canberra, Australia: National Health and Medical Research Council; 2000.
-
- OCEBM Levels of Evidence Working Group. "The Oxford 2011 Levels of Evidence". Oxford Centre for Evidence-Based Medicine; Available: http://www.cebm.net/index.aspx?o=5653.
-
- Higgins JPT, Altman DG, Sterne JAC. Chapter 8: Assessing risk of bias in included studies In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available: www.cochrane-handbook.org.
-
- Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA. 1995;273(5):408–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
