

Vitamin D serum level is associated with Child-Pugh score and metabolic enzyme imbalances, but not viral load in chronic hepatitis B patients
- PMID: 27399065
- PMCID: PMC5058794
- DOI: 10.1097/MD.0000000000003926
Vitamin D serum level is associated with Child-Pugh score and metabolic enzyme imbalances, but not viral load in chronic hepatitis B patients
Abstract
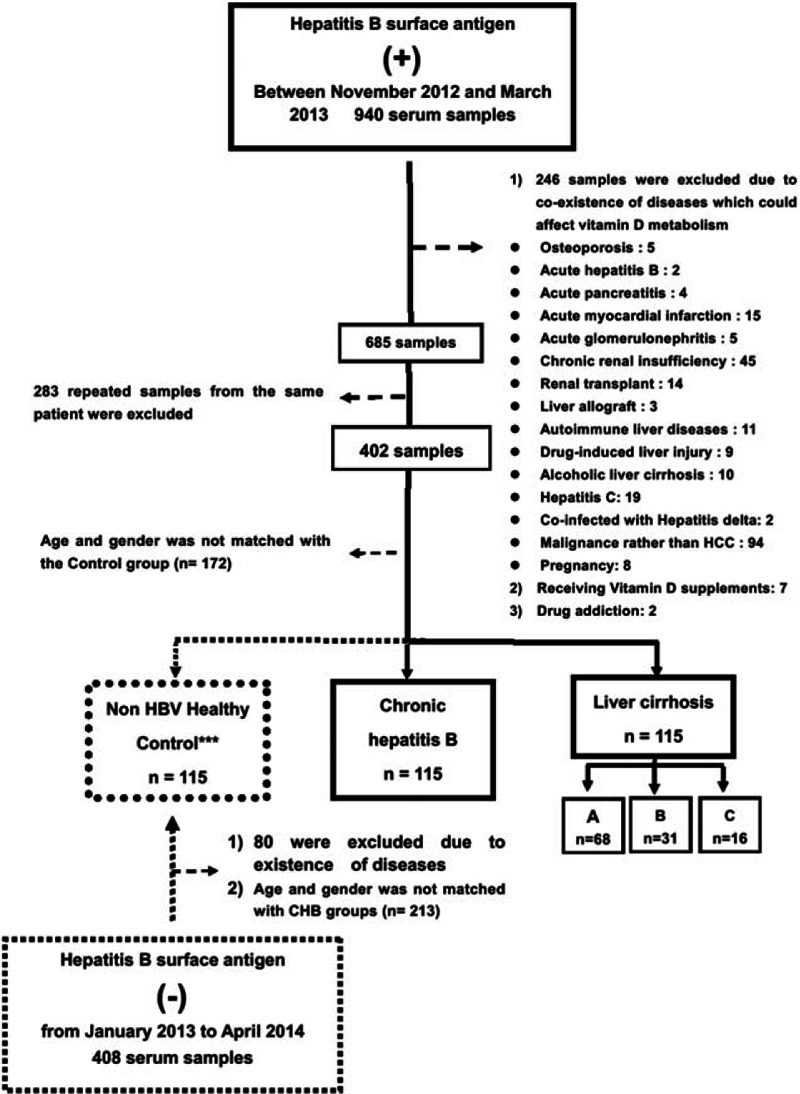
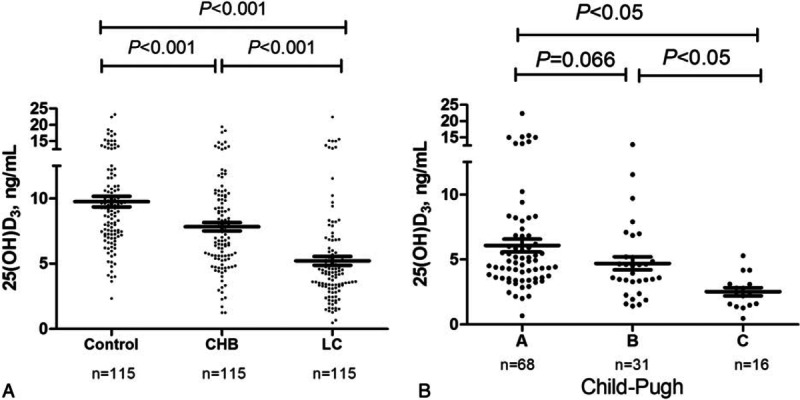
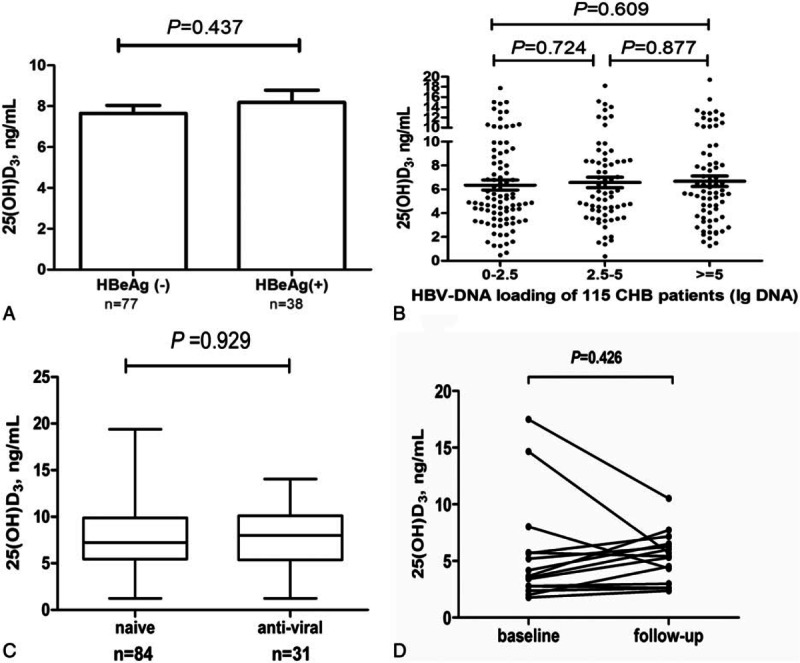
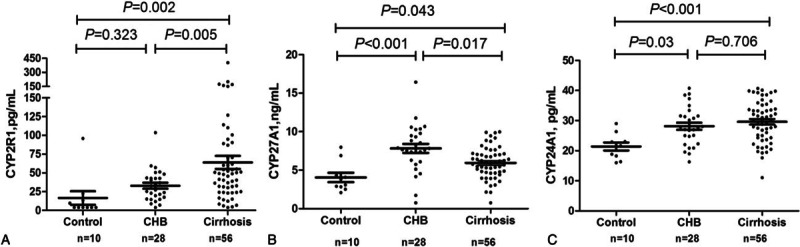
Vitamin D deficiency is common in patients with chronic liver diseases. However, vitamin D status in persons with chronic hepatitis B virus (HBV) infection is not consistently reported. Specifically, the impact of liver dysfunction on vitamin D status has not been well addressed.We recruited a group of patients (n = 345) with chronic hepatitis B (n = 115), hepatitis B related cirrhosis (n = 115), and age- and gender-matched healthy controls (n = 115). Serum 25-hydroxyvitamin D3 [25(OH)D3], its related metabolic enzymes, intact parathyroid hormone were measured. Calcium, magnesium, and phosphorus were obtained from medical record.Serum 25(OH)D3 levels in chronic hepatitis B patients (7.83 ± 3.47 ng/mL) were significantly lower than that in healthy controls (9.76 ± 4.36 ng/mL, P < 0.001), but significantly higher than that in hepatitis B-related cirrhotic patients (5.21 ± 3.67 ng/mL, P < 0.001). Furthermore, 25(OH)D3 decreased stepwise with higher Child-Pugh classification. However, there were no significant differences in 25(OH)D3 levels between (1) hepatitis B e antigen (HBeAg +) and HBeAg(-) persons, or (2) among persons with different HBV viral load, or (3) between treatment naïve and patients on antiviral therapy. Multiple logistic regression analyses confirmed that higher Child-Pugh score was independently associated with 25(OH)D3 deficiency (<10 ng/mL) with an odds ratio of 1.20 (confidence interval 1.03-1.39, P = 0.016). Levels of cytochrome P450 (CYP) 27A1 were significantly decreased, whereas levels of CYP24A1 were significantly elevated in cirrhotic patients.These results suggest that decreasing vitamin D levels are likely to be a result, rather than a cause, of liver dysfunction and irrespective of HBV viral load. Reduction in 25(OH)D3 levels is possibly due to downregulation of the synthetic hydroxylase CYP27A1 and concurrent upregulation of degrading CYP24A1 in patients with liver cirrhosis.
Conflict of interest statement
There is no conflict of interests to be declared from all authors.
Figures
References
-
- Kitson MT, Roberts SK. D-livering the message: the importance of vitamin D status in chronic liver disease. J Hepatol 2012; 57:897–909. - PubMed
-
- Agmon-Levin N, Kopilov R, Selmi C, et al. Vitamin D in primary biliary cirrhosis, a plausible marker of advanced disease. Immunol Res 2015; 61:141–146. - PubMed
-
- Ladero JM, Torrejon MJ, Sanchez-Pobre P, et al. Vitamin D deficiency and vitamin D therapy in chronic hepatitis C. Ann Hepatol 2013; 12:199–204. - PubMed
-
- Gerova DI, Galunska BT, Ivanova II, et al. Prevalence of vitamin D deficiency and insufficiency in Bulgarian patients with chronic hepatitis C viral infection. Scand J Clin Lab Invest 2014; 74:665–672. - PubMed
-
- Trepo E, Ouziel R, Pradat P, et al. Marked 25-hydroxyvitamin D deficiency is associated with poor prognosis in patients with alcoholic liver disease. J Hepatol 2013; 59:344–350. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
