

Outcomes of off- and on-hours admission in ST-segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention: A retrospective observational cohort study
- PMID: 27399103
- PMCID: PMC5058832
- DOI: 10.1097/MD.0000000000004093
Outcomes of off- and on-hours admission in ST-segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention: A retrospective observational cohort study
Erratum in
-
Erratum: Outcomes of off- and on-hours admission in ST-segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention: A retrospective observational cohort study: Erratum.Medicine (Baltimore). 2016 Sep 9;95(36):e5091. doi: 10.1097/01.md.0000494755.80250.91. eCollection 2016 Sep. Medicine (Baltimore). 2016. PMID: 31265638 Free PMC article.
Abstract
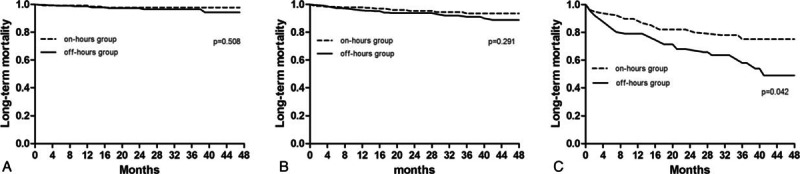
Studies evaluating the outcomes of patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI) are scarce, particularly in China. The purpose of present study was therefore to compare the impact of off-hours and on-hours admission on clinical outcomes in STEMI patients from China.We retrospectively analyzed 1594 patients from 4 hospitals. Of these, 903 patients (56.65%) were admitted during off-hours (weekdays from 18:00 to 08:00, weekends and holidays) and 691 (43.35%) were during on-hours (weekdays from 08:00 to 18:00).Patients admitted during off-hours had higher thrombolysis in myocardial infarction risk score (4.67 ± 2.27 vs 4.39 ± 2.10, P = 0.012) and longer door-to-balloon time (72 [50-96] vs 64 [42-92] minutes, P < 0.001) than those admitted during on-hours. Off-hours admission had no association with in-hospital (unadjusted odds ratio 2.069, 95% confidence interval [CI] 0.956-4.480, P = 0.060) and long-term mortality (unadjusted hazards ratio [HR] 1.469, 95%CI 0.993-2.173, P = 0.054), even after adjustment for confounders. However, long-term outcomes, the composite of deaths and other adverse events, differed between groups with an unadjusted HR of 1.327 (95%CI, 1.102-1.599, P = 0.003), which remained significant in regression models. In a subgroup analysis, off-hours admission was associated with higher long-term mortality in the high-risk subgroup (unadjusted HR 1.965, 95%CI 1.103-3.512, P = 0.042), but not in low- and moderate-risk subgroups.This study showed no association between off-hours admission and in-hospital and long-term mortality. Stratified analysis indicated that off-hours admission was significantly associated with long-term mortality in the high-risk subgroup.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Kostis WJ, Demissie K, Marcella SW, et al. Weekend versus weekday admission and mortality from myocardial infarction. N Engl J Med 2007; 356:1099–1109. - PubMed
-
- Gyenes GT, Yan AT, Tan M, et al. Use and timing of coronary angiography and associated in-hospital outcomes in Canadian non-ST-segment elevation myocardial infarction patients: insights from the Canadian Global Registry of Acute Coronary Events. Can J Cardiol 2013; 29:1429–1435. - PubMed
-
- Isogai T, Yasunaga H, Matsui H, et al. Effect of weekend admission for acute myocardial infarction on in-hospital mortality: a retrospective cohort study. Int J Cardiol 2015; 179:315–320. - PubMed
-
- Kumar G, Deshmukh A, Sakhuja A, et al. Acute myocardial infarction: a national analysis of the weekend effect over time. J Am Coll Cardiol 2015; 65:217–218. - PubMed
-
- Henriques JPS, Haasdijk AP, Zijlstra F. Outcome of primary angioplasty for acute myocardial infarction during routine duty hours versus during off-hours. J Am Coll Cardiol 2003; 41:2138–2142. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
