

Low Prognostic Nutritional Index (PNI) Predicts Unfavorable Distant Metastasis-Free Survival in Nasopharyngeal Carcinoma: A Propensity Score-Matched Analysis
- PMID: 27399281
- PMCID: PMC4939954
- DOI: 10.1371/journal.pone.0158853
Low Prognostic Nutritional Index (PNI) Predicts Unfavorable Distant Metastasis-Free Survival in Nasopharyngeal Carcinoma: A Propensity Score-Matched Analysis
Abstract
Background: Poor nutritional status is associated with progression and advanced disease in patients with cancer. The prognostic nutritional index (PNI) may represent a simple method of assessing host immunonutritional status. This study was designed to investigate the prognostic value of the PNI for distant metastasis-free survival (DMFS) in patients with nasopharyngeal carcinoma (NPC).
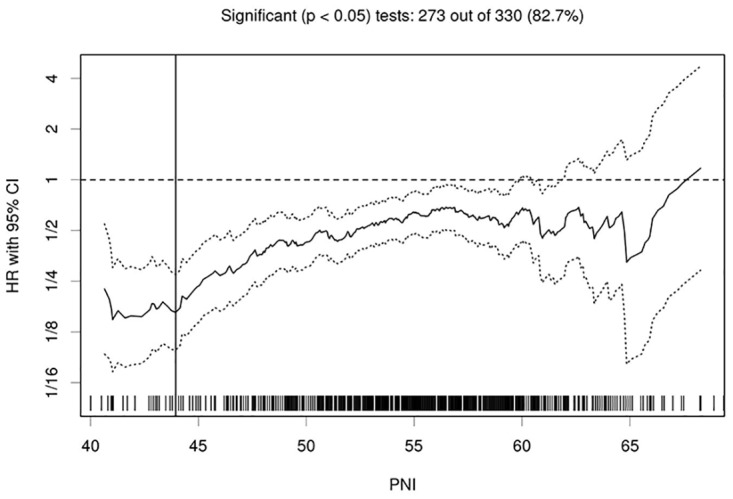
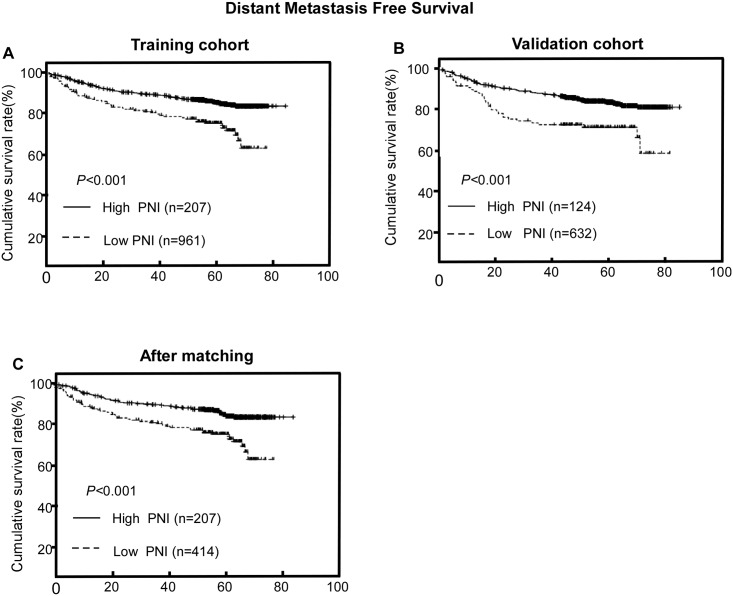
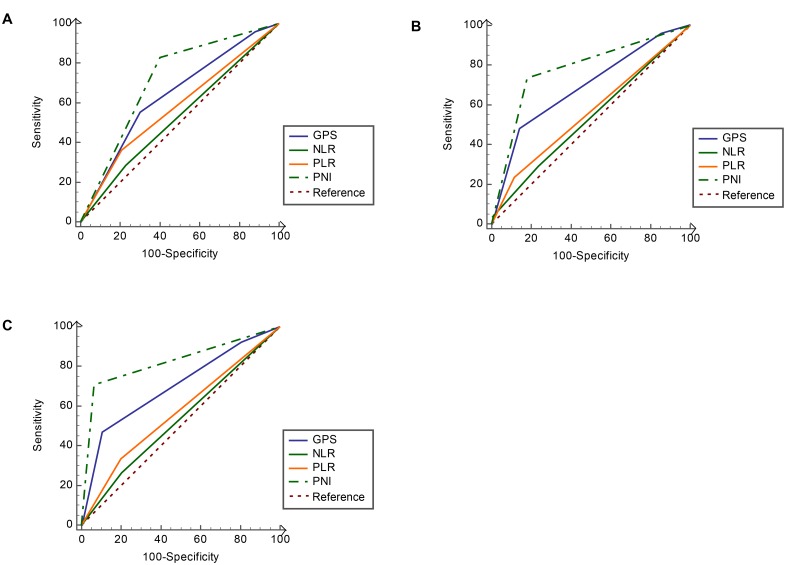
Methods: A training cohort of 1,168 patients with non-metastatic NPC from two institutions was retrospectively analyzed. The optimal PNI cutoff value for DMFS was identified using the online tool "Cutoff Finder". DMFS was analyzed using stratified and adjusted analysis. Propensity score-matched analysis was performed to balance baseline characteristics between the high and low PNI groups. Subsequently, the prognostic value of the PNI for DMFS was validated in an external validation cohort of 756 patients with NPC. The area under the receiver operating characteristics curve (AUC) was calculated to compare the discriminatory ability of different prognostic scores.
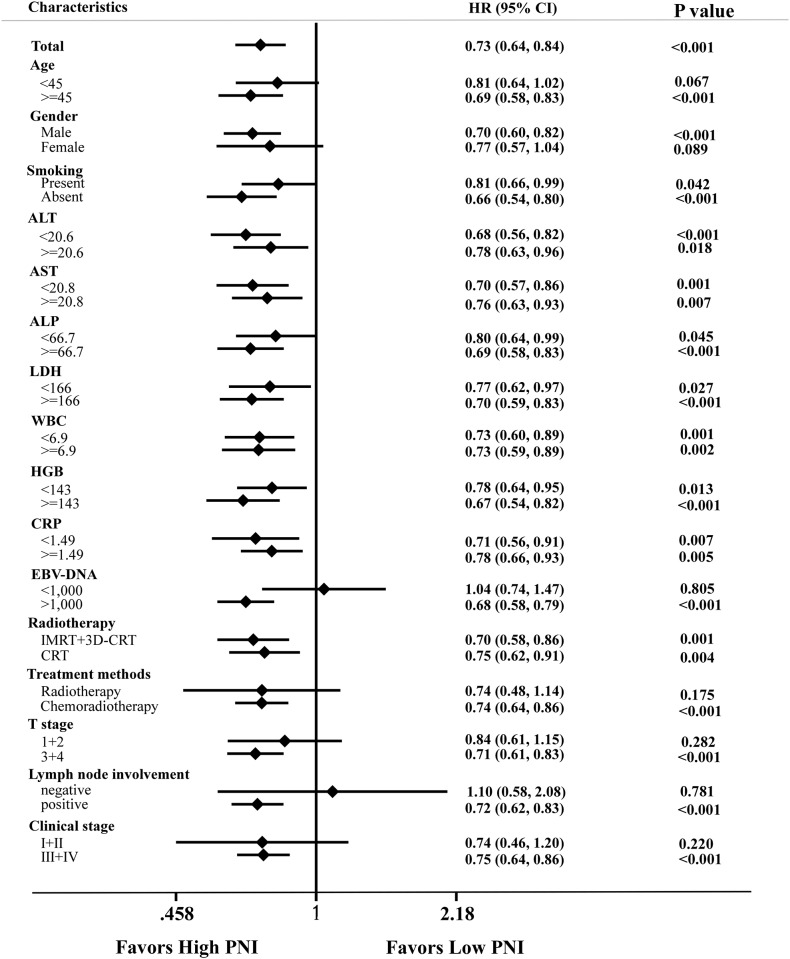
Results: The optimal PNI cutoff value was determined to be 51. Low PNI was significantly associated with poorer DMFS than high PNI in univariate analysis (P<0.001) as well as multivariate analysis (P<0.001) before propensity score matching. In subgroup analyses, PNI could also stratify different risks of distant metastases. Propensity score-matched analyses confirmed the prognostic value of PNI, excluding other interpretations and selection bias. In the external validation cohort, patients with high PNI also had significantly lower risk of distant metastases than those with low PNI (Hazards Ratios, 0.487; P<0.001). The PNI consistently showed a higher AUC value at 1-year (0.780), 3-year (0.793) and 5-year (0.812) in comparison with other prognostic scores.
Conclusion: PNI, an inexpensive and easily assessable inflammatory index, could aid clinicians in developing individualized treatment and follow-up strategies for patients with non-metastatic NPC.
Conflict of interest statement
Figures
Similar articles
-
High C-reactive protein/albumin ratio predicts unfavorable distant metastasis-free survival in nasopharyngeal carcinoma: a propensity score-matched analysis.Cancer Manag Res. 2018 Feb 21;10:371-381. doi: 10.2147/CMAR.S155604. eCollection 2018. Cancer Manag Res. 2018. PMID: 29503584 Free PMC article.
-
Prognostic value of pretreatment prognostic nutritional index and lactated dehydrogenase in locally advanced nasopharyngeal carcinoma patients.Ann Palliat Med. 2021 Apr;10(4):4122-4133. doi: 10.21037/apm-20-2033. Epub 2021 Mar 23. Ann Palliat Med. 2021. PMID: 33832314
-
Baseline Low Prognostic Nutritional Index Predicts Poor Survival in Locally Advanced Nasopharyngeal Carcinomas Treated With Radical Concurrent Chemoradiotherapy.Ear Nose Throat J. 2021 Feb;100(2):NP69-NP76. doi: 10.1177/0145561319856327. Epub 2019 Jun 10. Ear Nose Throat J. 2021. PMID: 31184210
-
The prognostic role of prognostic nutritional index in nasopharyngeal carcinoma: A systematic review and meta-analysis.Int J Clin Oncol. 2021 Jan;26(1):66-77. doi: 10.1007/s10147-020-01791-x. Epub 2020 Oct 7. Int J Clin Oncol. 2021. PMID: 33029749
-
Pretreatment prognostic nutritional index as a prognostic marker in head and neck cancer: a systematic review and meta-analysis.Sci Rep. 2021 Aug 24;11(1):17117. doi: 10.1038/s41598-021-96598-9. Sci Rep. 2021. PMID: 34429476 Free PMC article.
Cited by
-
Pretreatment low prognostic nutritional index and low albumin-globulin ratio are predictive for overall survival in nasopharyngeal cancer.Eur Arch Otorhinolaryngol. 2019 Nov;276(11):3221-3230. doi: 10.1007/s00405-019-05595-2. Epub 2019 Aug 10. Eur Arch Otorhinolaryngol. 2019. PMID: 31401760
-
Low prognostic nutritional index is associated with poor outcome in middle-aged and elderly patients with non-metastatic nasopharyngeal carcinoma: a retrospective cohort study.Support Care Cancer. 2022 Nov;30(11):8895-8904. doi: 10.1007/s00520-022-07286-x. Epub 2022 Jul 25. Support Care Cancer. 2022. PMID: 35879471
-
Objective evaluation of nutritional status using the prognostic nutritional index during and after chemoradiotherapy in Japanese patients with head and neck cancer: a retrospective study.Eur J Hosp Pharm. 2021 Sep;28(5):266-270. doi: 10.1136/ejhpharm-2019-001979. Epub 2019 Aug 17. Eur J Hosp Pharm. 2021. PMID: 34426479 Free PMC article.
-
A New Prognostic Parameter Associated With Recurrence in Patients With Nasopharyngeal Cancer Treated With Chemoradiotherapy: The Ratio of the Hemoglobin-to-Red Cell Distribution Width.Cureus. 2023 Jun 3;15(6):e39907. doi: 10.7759/cureus.39907. eCollection 2023 Jun. Cureus. 2023. PMID: 37404429 Free PMC article.
-
Pretreatment combination of platelet counts and neutrophil-lymphocyte ratio predicts survival of nasopharyngeal cancer patients receiving intensity-modulated radiotherapy.Onco Targets Ther. 2017 May 26;10:2751-2760. doi: 10.2147/OTT.S137000. eCollection 2017. Onco Targets Ther. 2017. PMID: 28603425 Free PMC article.
References
-
- Thompson MP, Kurzrock R. Epstein-Barr virus and cancer. Clin Cancer Res. 2004;10(3):803–21. - PubMed
-
- Lee AW, Sze WM, Au JS, Leung SF, Leung TW, Chua DT, et al. Treatment results for nasopharyngeal carcinoma in the modern era: the Hong Kong experience. Int J Radiat Oncol Biol Phys. 2005;61(4):1107–16. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
