

Duration of Oxytocin and Rupture of the Membranes Before Diagnosing a Failed Induction of Labor
- PMID: 27400012
- PMCID: PMC4959965
- DOI: 10.1097/AOG.0000000000001527
Duration of Oxytocin and Rupture of the Membranes Before Diagnosing a Failed Induction of Labor
Abstract
Objective: To compare maternal and neonatal outcomes based on length of the latent phase during induction with rupture of membranes before 6 cm dilation.
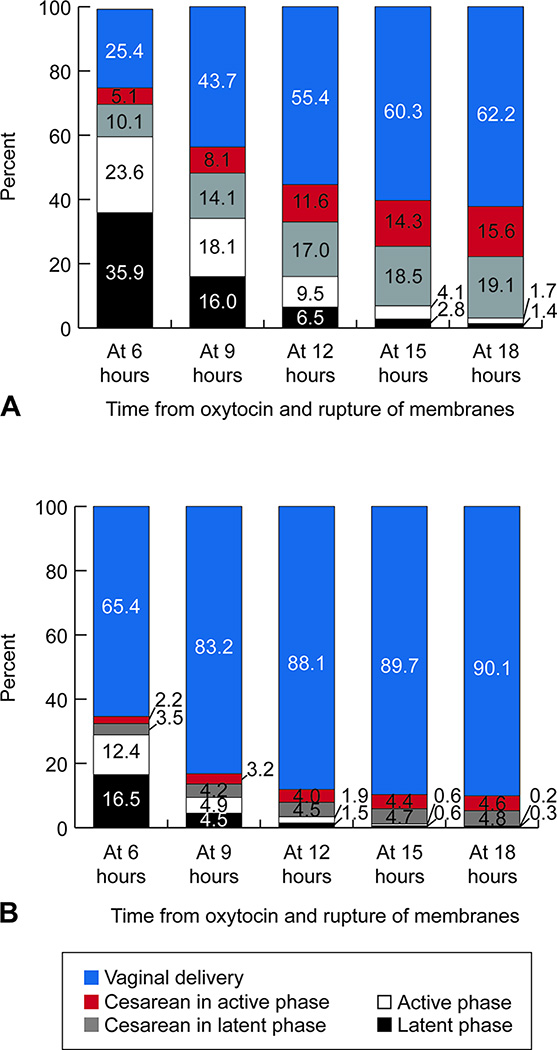
Methods: This is a retrospective cohort study using data from the Consortium of Safe Labor study, including 9,763 nulliparous and 8,379 multiparous women with singleton, term pregnancies undergoing induction at 2 cm dilation or less with rupture of membranes before 6 cm dilation after which the latent phase ended. Outcomes were evaluated according to duration of oxytocin and rupture of membranes.
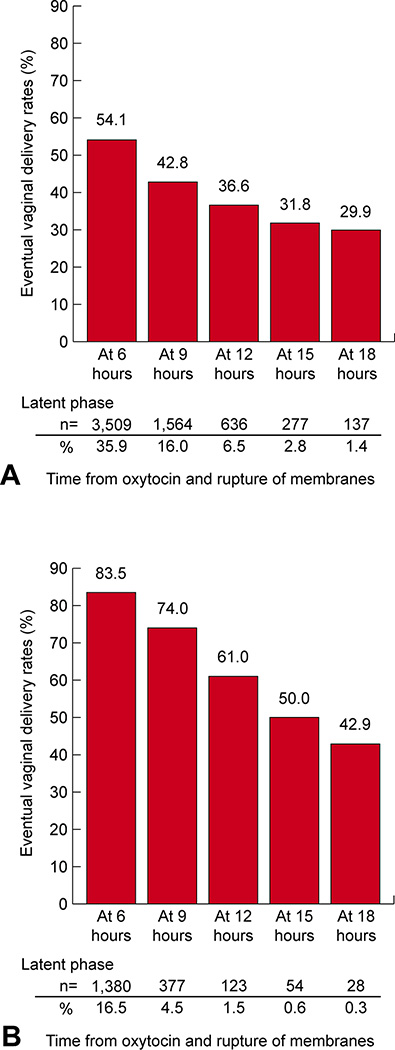
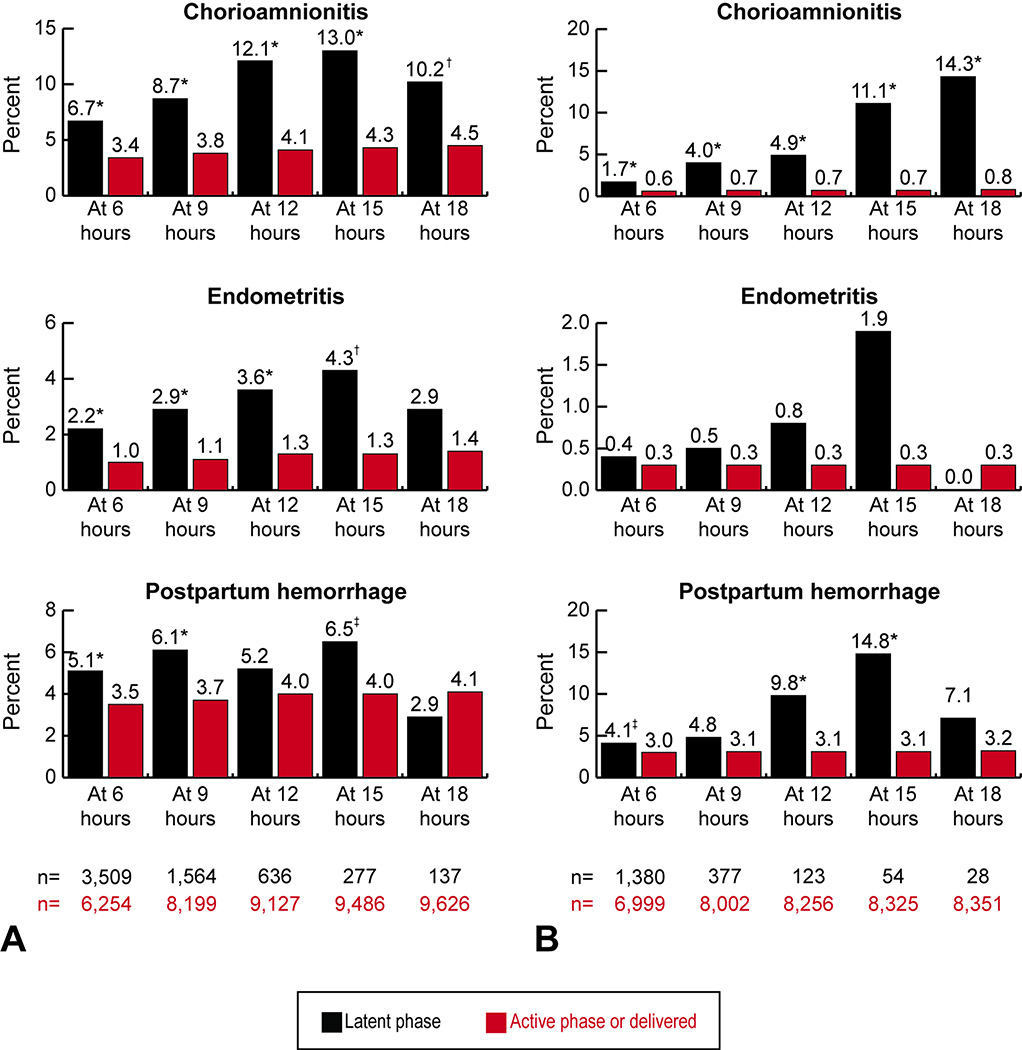
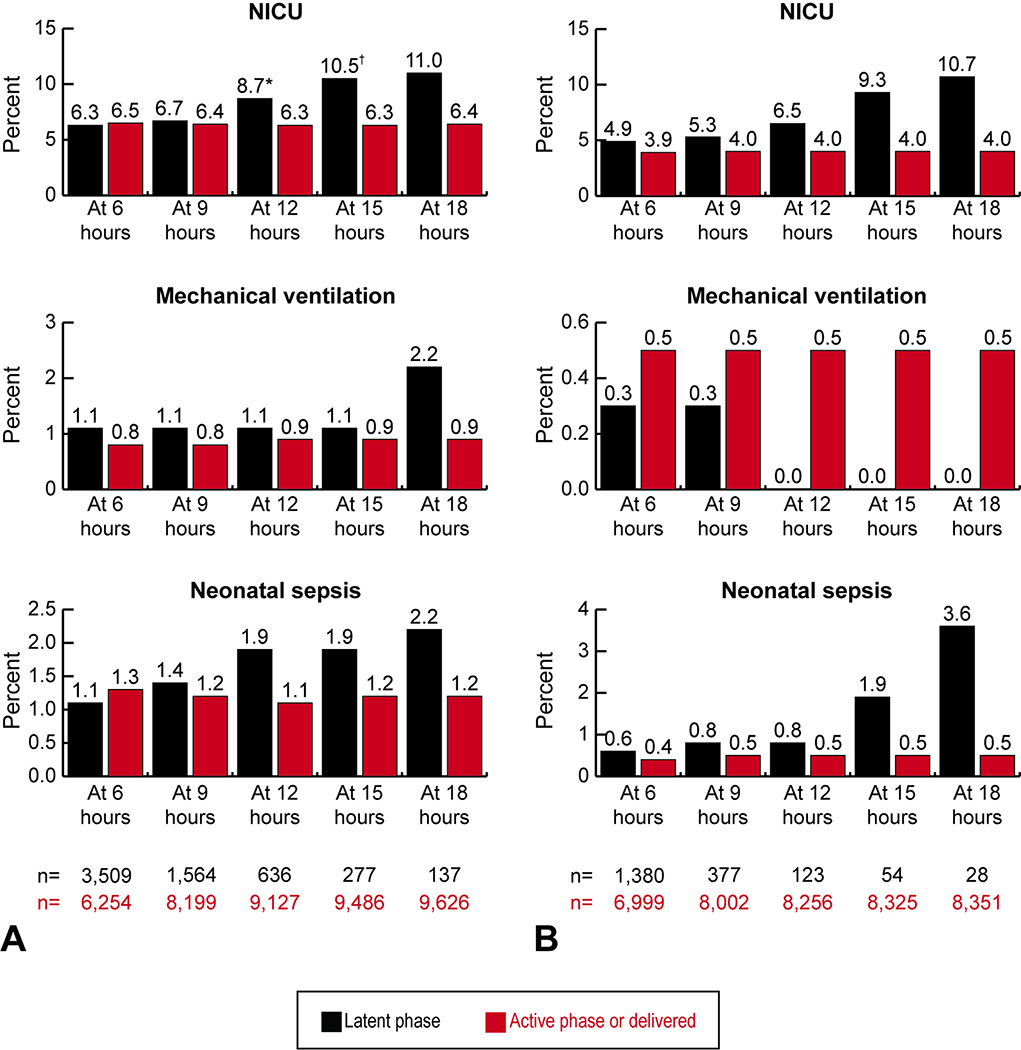
Results: At time points from 6 to 18 hours of oxytocin and rupture of membranes, the rates of nulliparous women remaining in the latent phase declined (35.9-1.4%) and the rates of vaginal delivery for those remaining in the latent phase at these time periods decreased (54.1-29.9%) Nulliparous women remaining in the latent phase for 12 hours compared with women who had exited the latent phase had significantly increased rates of chorioamnionitis (12.1% compared with 4.1%) and endometritis (3.6% compared with 1.3%) and increased rates of neonatal intensive care unit admission (8.7% compared with 6.3%). Similar patterns were present for multiparous women at 15 hours.
Conclusion: Based on when neonatal morbidity increased, in an otherwise uncomplicated induction of labor with rupture of membranes, a latent phase after initiation of oxytocin of at least 12 hours for nulliparous women and 15 hours in multiparous women is a reasonable criterion for diagnosing a failed induction.
Conflict of interest statement
The authors did not report any potential conflicts of interest.
Figures
Comment in
-
Duration of Oxytocin and Rupture of the Membranes Before Diagnosing a Failed Induction of Labor.Obstet Gynecol. 2016 Nov;128(5):1183. doi: 10.1097/AOG.0000000000001729. Obstet Gynecol. 2016. PMID: 27776060 No abstract available.
-
In Reply.Obstet Gynecol. 2016 Nov;128(5):1183. doi: 10.1097/AOG.0000000000001730. Obstet Gynecol. 2016. PMID: 27776061 No abstract available.
References
-
- Martin JA, Hamilton EB, Osterman JK, Curtin SC, Mathews TJ. Centers for Disease Control and Prevention National Center for Health Statistics National Vital Statistics System. Births: final data for 2013. Natl Vital Stat Rep. 2015;64(1):1–68. - PubMed
-
- Rouse DJ, Weiner SJ, Bloom SL, Varner MW, Spong CY, Ramin SM, et al. Failed labor induction: toward an objective diagnosis. Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU) Obstet Gynecol. 2011;117:267–272. - PMC - PubMed
-
- American College of Obstetrics and Gynecologists; Society for Maternal-Fetal Medicine. Safe prevention of the primary cesarean delivery. Am J Obstet Gynecol. 2014;210(3):179–193. - PubMed
-
- Rouse DJ, Owen J, Hauth JC. Criteria for failed labor induction: Prospective evaluation of a standard protocol. Obstet Gynecol. 2000;96:671–677. - PubMed
-
- Simon CE, Grobman WA. When has an induction failed? Obstet Gynecol. 2005;105:705–709. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
